Peptides 101 is the conceptual intro. This is the cycle-planning piece you read after, when the question turns from "what is this stuff" to "OK I'm running one, what am I actually doing." First cycles fail more often than they should, and the failures are usually predictable. This article walks the choices in order, names the most common mistakes, and ends with what a 4-week reassessment looks like.
The honest setup before any of this
A first peptide cycle competes with cheaper, better-tested interventions. Sleep, training, protein intake, and lifting load produce more body-composition change than any peptide for most users at most baselines. If you're not already getting most of the value those produce, a peptide cycle is a small lever on top of a missing big one. That's not a moralistic point - it's that the marginal effect of a cycle is hard to detect against a noisier baseline.
The audience this site is written for has typically already done that work. The article assumes that. If you haven't yet, run a 3-month sleep + training + protein discipline pass first; the cycle-planning conversation gets cleaner once those are stable.
Step 1: pick exactly one goal
The single most common first-cycle mistake is stacking goals. "Fat loss + recovery + better sleep + maybe some hair benefit" is not a cycle plan. It's a wishlist. Each goal points to a different compound class with a different protocol, and stacking three at once means you can't tell which - if any - of them is working.
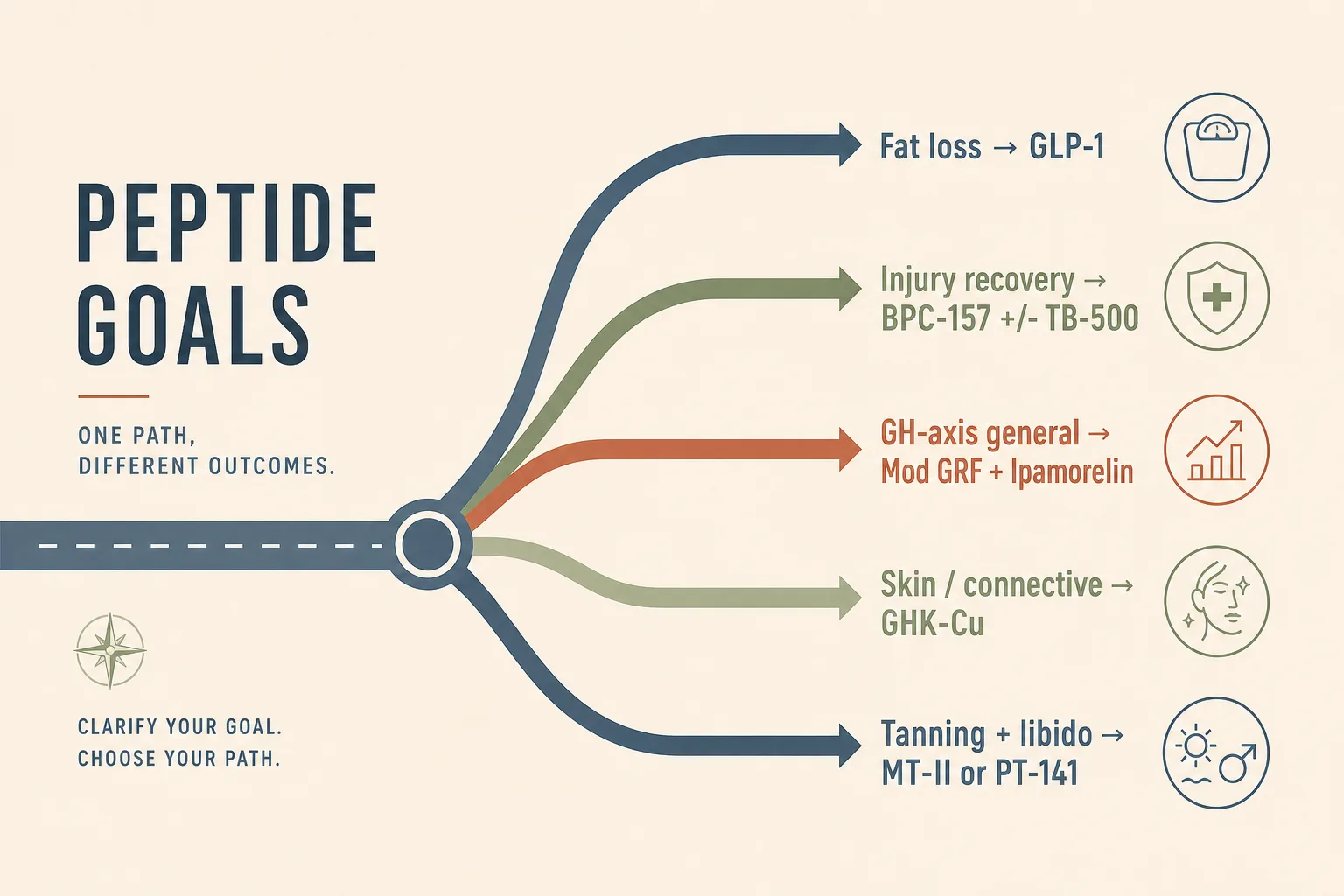
- Fat loss. If you have meaningful body fat to lose and an established calorie deficit, a GLP-1 receptor agonist (semaglutide or tirzepatide via approved channels) is the highest-evidence first cycle in this space. See Semaglutide vs Tirzepatide vs Retatrutide.
- Soft-tissue injury or post-surgical recovery. BPC-157 alone, or BPC + TB-500 if multi-site. Local injection near the injury for BPC. See Injury Recovery; for the surgical-context branch (pre-op set-up window, anesthesia washout, post-op timing) see Peptides Around Surgery.
- Sleep, recovery feel, body-composition optimisation on a stable training base. Pulsatile GH-axis stack: Mod GRF + Ipamorelin pre-bed. The cleanest first GH-axis cycle. See GH Axis Playbook.
- Skin and connective tissue. GHK-Cu topical is the lowest-stakes entry point; systemic if connective tissue is the priority. See Skin and Hair.
- Tanning + libido package. Melanotan II if you specifically want both. PT-141 if just libido. The melanocortin map sorts these by receptor selectivity: Melanocortin Map.
Pick one. The other goals don't disappear; they go on the next-cycle list once you've finished the first one and can reason about it cleanly.
Step 2: pick the compound and confirm the protocol
With the goal narrowed, the compound class follows. Read the dedicated peptide page for the compound you've chosen and read the application page for the goal it sits in. Both pages exist for a reason. The compound page tells you the mechanism, dosing and protocol; the application page tells you how it fits in a realistic stack and what the alternatives are.
- Read the peptide page end to end. The "common cautions" section is where the things that surprise first-cycle users live. Don't skip it.
- Confirm the dose and route. Cross-check against the application page; community forum protocols sometimes differ from the operator-grade reference here, often on the unsafe side.
- Confirm the cycle length. Most first cycles are 4-8 weeks. Open-ended "I'll run it as long as it feels good" is a setup for cumulative-exposure problems. See Cycling Strategies.
Step 3: source quality is non-negotiable
Source quality is the most common cause of first-cycle failure. Protocols don't work on bunk or underdosed material. Don't skip this step.
- Use the prescription channel where one exists. GLP-1 family compounds, tesamorelin, somatropin (with a real diagnosis), Vyleesi (PT-141), Scenesse (Melanotan I) all have approved channels somewhere. The off-label premium is often less than the cost of multiple grey-market verification rounds.
- If grey-market is the only option, test the first vial. HPLC + mass spec from a third-party peptide- testing lab. Costs $80-200; pays for itself the first time it catches a problem. See Sourcing and Verification and the decoder companion Understanding Peptide Purity.
- Order supplies separately. Sterile bacteriostatic water from a pharmacy or medical-supply vendor, not from the peptide vendor. Insulin syringes (1 mL with 30G or smaller needles for SC), alcohol wipes, sharps container.
Step 4: baseline measurements (don't skip)
Cycle outcomes are unintelligible without baseline data. The first-cycle user who skips this can't distinguish "the peptide worked" from "the diet finally locked in" from "I started sleeping better in the same window." Three categories of baseline matter:
- Bloodwork. CBC + CMP + lipids + HbA1c + IGF-1 minimum. The full per-class panel and timing rules are in Bloodwork for Peptide Users. Self-pay packages run $80-150; the cost is a fraction of the cycle.
- Body composition. Photo (front, side, back) in the same lighting and clothing. DEXA or bioimpedance if accessible; tape measurements at consistent landmarks if not. Done once before starting and once at the end is enough; weekly is better.
- Resting heart rate and (if you have a wearable) HRV. Two weeks of morning measurements before the cycle starts. Average, not single number. See Heart Rate as a Peptide Sentinel.
These are not optional. The user who runs a cycle without baseline ends up with a subjective impression of "I think I feel better" or "I don't think anything happened" that's uninformative and irreproducible. The data is what makes the next cycle decision tractable.
Step 5: run the protocol with discipline
The protocol is whatever the dedicated peptide page says it is. Run it as written for the first cycle. Don't innovate.
- Hold the timing. GH-axis stacks need a fasted window. GLP-1s have a step-up schedule. MT-II has a loading phase. The timing isn't a suggestion; it's part of the protocol. See Peptides and Insulin for the fasting-window mechanism.
- Reconstitute carefully and confirm the dose math. A 5 mg vial reconstituted with 2 mL gives 2.5 mg/mL = 250 mcg per 0.1 mL. Confirm before drawing. See Syringe-Draw Dosage Math.
- Rotate injection sites. Abdomen, thigh, deltoid, glute. Not the same spot twice in a row. See Injection Rotation.
- Store the vial correctly. Refrigerator after reconstitution; lyophilised powder room-temp short-term or fridge long-term. See Storage and Handling and the operator quick-reference Cold Chain Quick Reference.
- Keep a daily log. Date, time, site, dose, vial lot, and one-line subjective note. Three minutes a day. Saves hours of "did I dose Tuesday?" reconstruction later and makes the reassessment intelligible.
Step 6: the 4-week reassessment
Most cycles run 4-8 weeks; the 4-week mark is the natural reassessment milestone. Here's what to look at:
- Pull the bioassay where one exists. IGF-1 at 4-6 weeks for GH-axis cycles. Body-comp trend for GLP-1. Pigmentation / flushing trajectory for MT-II. If the bioassay didn't move, you have a sourcing or protocol problem - see When a Peptide Cycle Fails.
- Check the metabolic sentinels. Fasting glucose, HbA1c if applicable, resting heart rate trend. Drift outside expected ranges means dose down or pause; on track means continue.
- Compare body-comp photo or measurement to baseline. 4 weeks is enough to see directional movement on most cycles, especially GLP-1. If nothing has changed, the diet/training side may be the limiter, not the peptide.
- Audit subjective changes against the daily log. Sleep quality, recovery, energy, libido - sift these against the log notes, not retrospective memory. Memory is unreliable over a 4-week window.
- Decide: continue, dose-adjust, or stop. Continue if the bioassay and sentinels are on track. Adjust dose if you're at the bottom of the range and underperforming. Stop if a sentinel has drifted into stop-signal territory or the bioassay is flat-line.
What stops first-cycle users
- Stacking goals from day one. GLP-1 + BPC-157 + Mod GRF + GHK-Cu in your first cycle is four compounds, four protocols, and four bioassays you have to track and cross- correlate. Run one. Validate it. Add the next on cycle two.
- Picking the cheapest grey-market vendor without testing. The lowest-priced vial is usually the lowest-quality vial. The third-party test cost is not the place to optimise.
- Skipping baseline bloodwork. The first cycle is the cheapest to baseline because no compound is yet in the system. Skipping it is throwing away the cleanest comparison point you'll ever have.
- Innovating on the protocol. Halving the dose "to be safe" or doubling it "to feel something" both produce uninformative results. Run the standard protocol. Adjust on cycle two with data from cycle one.
- Treating the cycle as the lever. Sleep, training and food are still doing 80% of the work. The cycle is a multiplier on top, not a replacement.
- No cycle log. "I think I dosed Tuesday and Friday" is not protocol adherence data. The log is two minutes a day; without it the reassessment is fiction.
What this article doesn't cover
AAS-context first cycles (peptides on top of an existing AAS or TRT protocol) carry their own decision tree and are covered in Peptides on Top of an AAS or TRT Stack. Female-physiology-specific first-cycle considerations (cycle-phase interaction, PCOS context, perimenopausal hormone shifts) are in Peptides and Female Physiology. Pediatric and adolescent use is not in scope at all - the audience this site is written for is adult.
Cross-references
- Peptides 101 - the conceptual entry point this article assumes.
- Sourcing and Verification - the source-quality discipline this article leans on.
- Bloodwork for Peptide Users - the panel and timing for the baseline and follow-up draws.
- Syringe-Draw Dosage Math - the reconstitution and drawing math the protocol step depends on.
- Cycling Strategies - the on/off rationale that determines cycle length.
- When a Peptide Cycle Fails - the diagnostic to run if the reassessment finds nothing happening.