The peptides in this catalog are mostly grey-market goods. The ones that aren’t - Semaglutide, Tirzepatide, Tesamorelin, FDA-approved Scenesse, FDA-approved Vyleesi - have a clean prescription channel that solves the verification problem on your behalf. Everything else gets shipped from a contract manufacturer somewhere abroad, through a reseller who may or may not have ever opened the box, into a vial that may or may not contain what the label claims. This article walks through how to actually evaluate source quality without naming vendors (which would be wrong on legal, regulatory, and community-trust grounds).
Three things can be wrong with the vial
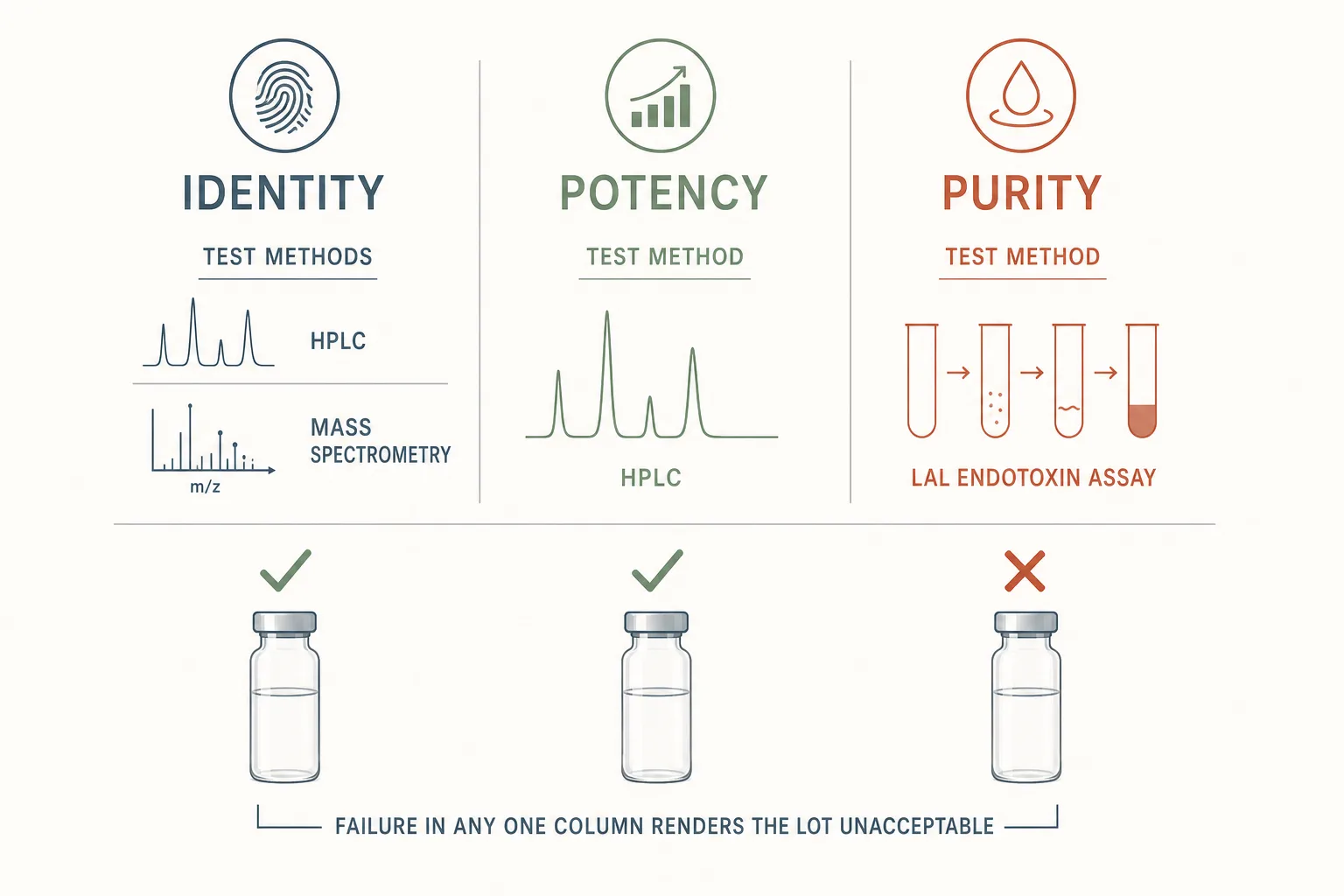
- Identity - the contents aren’t the peptide on the label. Could be a different peptide, a different molecule entirely, or nothing biologically active. Most catastrophic and rare in established networks; common in cheapest-tier listings.
- Potency - the peptide is correct but underdosed. This is the most common failure mode and the easiest to miss because the user just sees “weak response, must need more.”
- Purity - correct peptide at the right amount, but with contaminating peptides, residual solvents, endotoxin, or bacterial load above safe injection limits.
No single test catches all three. A complete verification pass needs identity (HPLC + mass spec), potency (quantification on the same HPLC run), and purity / endotoxin (LAL or recombinant Factor C assay). Most third-party labs offer the first two as a standard package; endotoxin is a separate add-on and worth paying for on injectables you plan to run for more than a one-off.
Third-party testing - what you’re actually paying for
A reputable peptide-testing lab will, for around $80–$200 per sample, run reverse-phase HPLC against a known standard for the target peptide, integrate the main peak as a percent of total absorbance, run mass spectrometry to confirm the molecular weight matches the expected mass, and report both as a certificate of analysis (COA). That COA is the only document that means anything. A vendor saying “tested” without a COA is saying nothing.
- Read the COA, don’t skim it. Check the peptide name and lot number on the COA against your vial. Lot mismatch is a red flag big enough that the rest of the document doesn’t matter.
- Mass spec confirms identity, HPLC main-peak percent confirms purity, area under the peak vs. standard confirms potency. All three should be on the same document for the same lot.
- >98% main-peak by HPLC is the practical floor. 95–98% is weak; below 95% is bunk-adjacent and the “impurity” column may be the interesting one (related peptides, oxidation products, or worse). What that number actually counts, why it means different things on a 5-mer vs a 35-mer, and what's in the missing 2% is broken out in Understanding Peptide Purity.
- Vendor-supplied COAs are not independent. A vendor running their own HPLC is a positive signal but not a substitute for sending a vial to a lab the vendor doesn’t pay. The cheapest reliable way to do this is to test one vial out of every new batch you order.
Bioassays - what your body confirms for free
For some peptide classes, your physiology runs a free verification assay every time you inject. The signal is weaker than HPLC but it’s real, repeatable, and catches the “underdosed” failure mode that paper testing sometimes misses if the lab tests a different vial than what you actually injected.
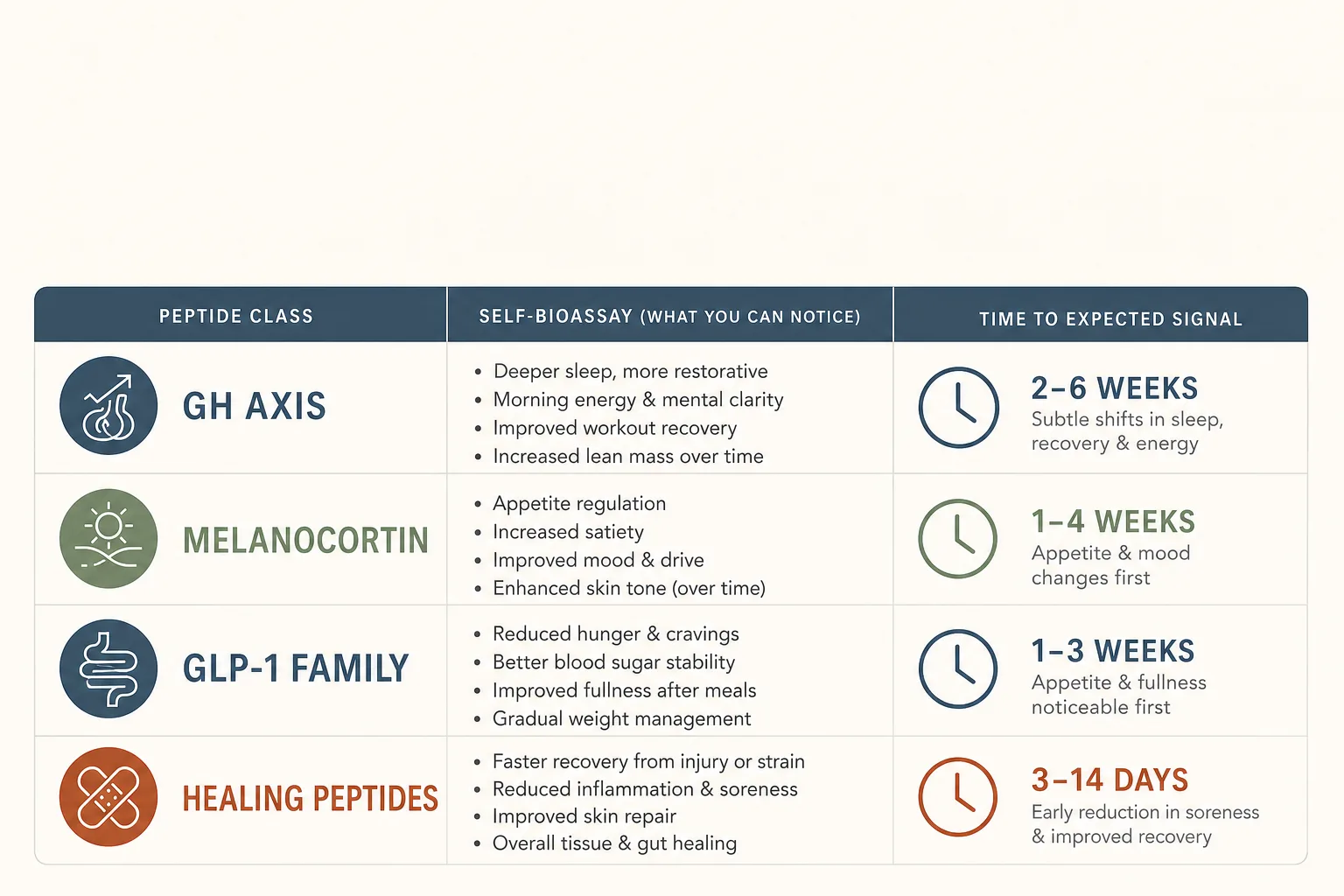
- GH axis (Mod GRF, CJC-1295, Ipamorelin, Tesamorelin, Somatropin): IGF-1 bloodwork at baseline and 6–8 weeks. CJC-1295 (DAC) and Somatropin should move the number meaningfully; pulsatile GHRH/GHRP stacks move it modestly. No move at all = the peptide is dead. See Bloodwork for Peptide Users.
- Melanocortin agonists (Melanotan II, PT-141, Melanotan I): a real MT-II produces unmistakable flushing and pigmentation response within the first 1–2 doses. PT-141 produces a real central effect within 45–90 minutes. Absence of either at expected doses is suspicious for an inert vial.
- GLP-1 family (Semaglutide, Tirzepatide, Retatrutide): appetite suppression is the bioassay. A real compound at a non-trivial dose (1 mg+ semaglutide, 5 mg+ tirzepatide, 4 mg+ retatrutide) produces measurable food-noise reduction within the first week. No effect after a full titration step = test the vial or change source. HbA1c and weight are slower confirmations.
- Healing peptides (BPC-157, TB-500, GHK-Cu): there is no clean bioassay. Subjective “I feel better” is not a verification signal. Rely on HPLC for these.
Vendor red flags
- No COA on request. A vendor unwilling or slow to share a COA for a specific lot is signaling something. Move on.
- COA without a lot number, or the same COA for every lot. A COA is a per-lot document. A “sample COA” that’s reused across batches is marketing, not testing.
- Prices materially below the market floor. A real peptide produced at pharmaceutical-adjacent purity has a manufacturing cost. Vendors selling at half the going rate are either taking a loss for customer acquisition (rare and short-lived) or are selling something that costs less to make than a real lot would.
- Aggressive medical claims. A vendor making efficacy claims is one that is going to get a warning letter and disappear, taking your forward-shipping credit with them.
- Vague or absent shipping practices. Lyophilized peptides survive room temperature for the duration of normal international shipping; reconstituted ones don’t. Vendors who can’t articulate this distinction are not a serious operation.
- Pressure to switch to crypto-only or off-platform payment after first contact. Some legitimate vendors do crypto-only by default; the red flag is pressure to leave a recoverable channel after engagement.
- Forum reputation that’s less than two years old. Reseller networks rotate brands; an account “everyone is happy with” that’s fresh is often the same operator who burned the previous brand.
Reconstitution and water hygiene
Even a perfect lot can become a contaminated lot in your kitchen. The hygiene rules are cheap and worth following exactly:
- Bacteriostatic water (0.9% benzyl alcohol) for anything you’ll keep in the fridge for more than 24 hours after reconstitution. Plain sterile water is fine for single-day use only.
- Wipe the vial septum with isopropyl alcohol before every draw. Once is not enough; every time.
- Don’t pierce the septum more than ~25 times. Past that the rubber starts to fragment and contamination risk climbs steeply.
- Use a fresh syringe per draw. Reusing the same needle to pierce the vial repeatedly is a contamination vector that’s easy to fix.
- Refrigerate reconstituted vials at 2–8 °C. Don’t freeze unless you specifically know the peptide tolerates a freeze-thaw (most do not).
See Reconstitution Fundamentals for the actual procedure and Storage and Handling for stability windows by class.
The buying stack people actually run
- Use the prescription channel where one exists. Semaglutide, tirzepatide, tesamorelin, Vyleesi, Scenesse, somatropin (with a real diagnosis): if the approved version is accessible at any price, that’s the verification problem solved. The off-label cost premium is often less than the cost of testing several grey-market vials yourself.
- Test one vial out of every new batch. Send to a third-party peptide-testing lab; pay for HPLC + MS at minimum. Endotoxin add-on for anything you’ll inject more than a few times. Keep COAs in the same folder as your bloodwork.
- Cross-check the lot with bioassay where available. IGF-1 bloodwork on a GH-axis cycle is a free verification you should be running anyway.
- Stay with one or two vendors past the trial-and-error phase. Switching constantly multiplies the verification load. A vendor who has held up across several COA batches becomes a real operational asset; treat that relationship accordingly.
- Don’t hoard. Lyophilized peptide has a long shelf life, but market dynamics, supply chains, and your goals all change. Buy quarterly, not yearly.
What this article doesn’t cover
Specific vendor recommendations are out of scope. They are out of scope on legal grounds (FDA enforcement varies by jurisdiction), trust grounds (any list this article ships becomes the target the next round of bad actors imitates), and durability grounds (vendor rotation cycles in this market are measured in months, not years). The community-forum reputation channels are imperfect but they are the actual answer to the “who right now” question. Counterfeit detection beyond HPLC + MS - isotope-ratio mass spectrometry, peptide-mapping LC-MS/MS - is laboratory-grade work and a separate topic. Compounding-pharmacy semaglutide and tirzepatide sourcing has its own regulatory complications and warrants its own writeup.