Soft-tissue injuries - tendon, ligament, partial muscle tears - are the application that built the peptide community’s reputation. The default healing pair, BPC-157 plus TB-500, has been around long enough that user reports are now in their second decade, and the case for it is strong even where the formal trial data is thin. This page covers when each compound matters, how to pick local vs systemic injection, when the GH axis is worth adding, and what to expect from a real recovery cycle.
This is not a substitute for a rehab program. Tissue healing without progressive loading produces tissue that scars rather than regenerates. The peptides shorten the timeline and improve the quality of the repair; they don’t replace the work.
The default pair
BPC-157 - local healing, gut adjunct
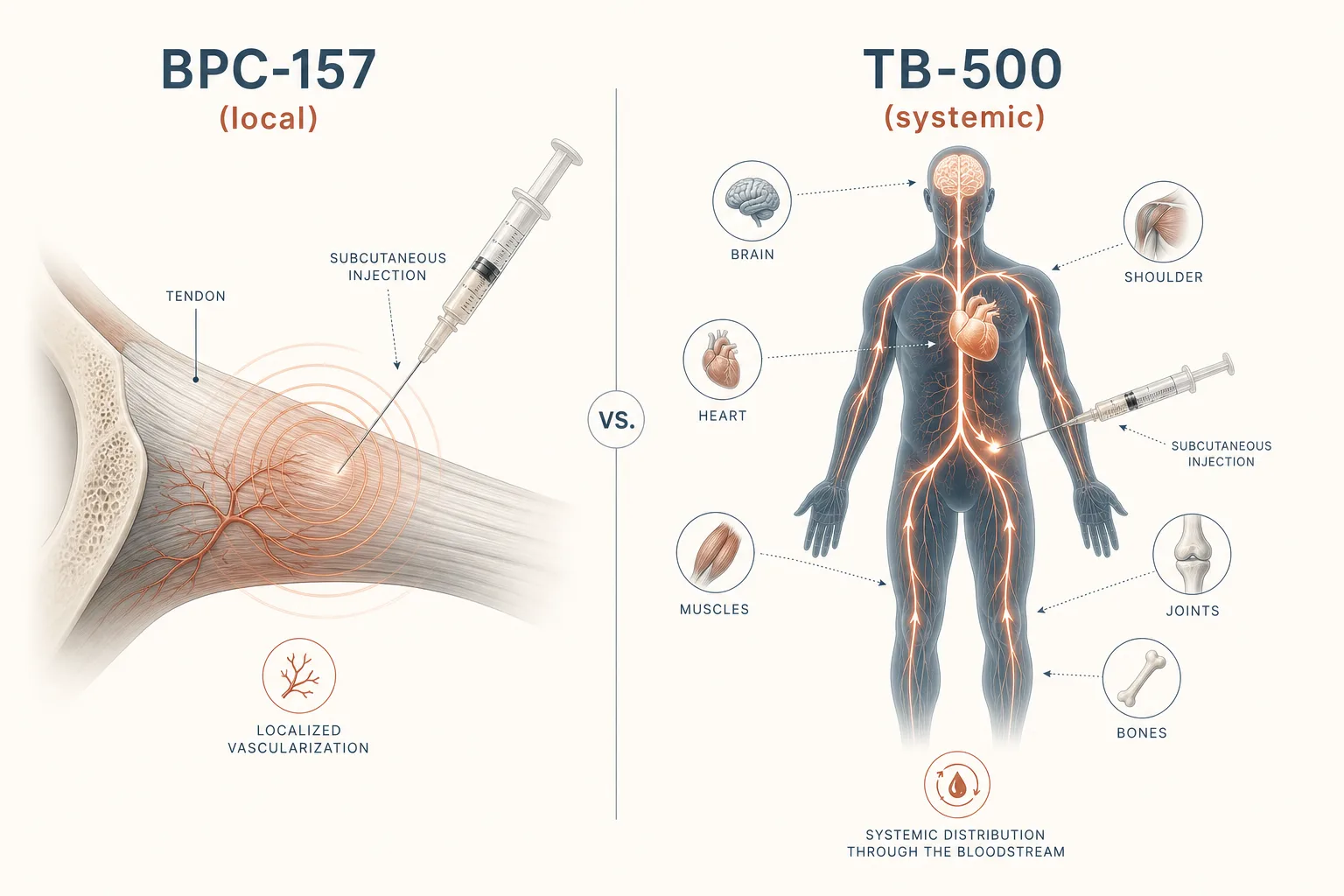
- Mechanism: upregulates VEGF and fibroblast migration, modulates the nitric-oxide pathway. The result is faster vascularization of poorly perfused tissue (tendons, ligaments) and accelerated structural repair.
- Default protocol: 250–500 mcg subcutaneous once or twice daily, 4–8 weeks. Inject as close to the injury site as is anatomically reasonable; the local effect is real and measurable.
- Local vs systemic: for a localized soft-tissue problem - one tendon, one joint - injection near the site outperforms a remote site. For diffuse or systemic issues, anywhere subcutaneous works.
- Oral form: oral BPC-157 (capsules, sometimes called “BPC-157 Arginate”) is real and useful specifically for gut-related issues - leaky-gut symptoms, NSAID-induced gut damage, IBD-adjacent inflammation. It does not deliver enough to the systemic circulation to drive joint healing on its own; use the injectable for that.
TB-500 - systemic healing, cell migration
- Mechanism: the LKKTETQ fragment of Thymosin Beta-4. Sequesters G-actin and promotes endothelial cell migration; net effect is angiogenesis plus accelerated cell migration to injury sites.
- Default protocol: a loading phase of 4–5 mg per week, split into twice-weekly subcutaneous injections, for the first 4–6 weeks. Maintenance at 2–2.5 mg per week thereafter, until function is restored.
- Local vs systemic: TB-500 is the systemic player. Site of injection matters less; it goes where there’s damage by following inflammatory signaling. Useful for multi-site issues, soft-tissue plus a connective-tissue overlap, or anything you can’t pin to one location.
BPC-157 and TB-500 stack synergistically. The default soft-tissue protocol is both together: BPC-157 250 mcg twice daily near the injury, TB-500 5 mg/week loading. After 4 weeks, drop to BPC-157 once daily and TB-500 maintenance until functional return. The mechanism story behind the synergy - why each compound rate-limits a different step of the proliferation phase, where the synergy thesis weakens, and the four-row use-case timing table - is in BPC-157 + TB-500: The Synergy Story Beyond the Headlines.
Adding the GH axis
For older users, slow-healing tissues, or aggressive return-to-sport timelines, adding a pulsatile GH-axis stack on top of BPC + TB-500 is the next move. The mechanism overlap is partial - BPC drives local vascularization, TB-500 drives migration, GH/IGF-1 drives the actual anabolic synthesis of new collagen. The three are complementary, not redundant.
- Default GH-axis addition: Mod GRF 1-29 100 mcg + Ipamorelin 100–200 mcg, pre-bed and optionally post-workout. See GH Axis Playbook for why this pairing.
- What it adds: a meaningful IGF-1 bump during the healing window, which is when collagen synthesis is actually happening. Rough rule: shaves 20–30% off recovery timelines for soft-tissue injuries when added on top of BPC + TB-500, more in older or under-recovered users.
- What it doesn’t replace: still need the BPC for local vascularization and the TB-500 for migration. GH-axis alone is a slower, less targeted approach.
Tertiary peptides
- GHK-Cu - topical for surface wounds and skin healing; systemic for connective-tissue and broad anti-inflammatory tone. Adjunct rather than primary in injury contexts.
- Thymosin Beta-4 (parent of TB-500) - full-length molecule, used in some protocols where the LKKTETQ fragment is judged insufficient. Practically, the fragment is what most people run.
- Thymosin Alpha-1 - not a healing peptide directly, but useful in injuries with chronic-inflammation or immune-component overlay (autoimmune-flare-driven joint pain, post-viral musculoskeletal issues). Don’t add it without a specific reason.
- IGF-1 LR3 - can drive local hypertrophy / structural buildup at injection sites. Usually deferred to the lean-mass-hypertrophy application; injury contexts with deconditioning are an exception.
Decision guide
- Localized soft-tissue injury (one tendon, one joint), no systemic
component?
→ BPC-157 alone, injected near the site, 4 weeks. Add TB-500 if no meaningful improvement by week 3. - Multi-site, diffuse, or unclear-localization issue?
→ BPC-157 systemic + TB-500 loading. Default 8–12 weeks. - Older user, aggressive timeline, or known slow healer?
→ Default pair plus pulsatile GH-axis stack. Add the Mod GRF + Ipamorelin pre-bed. - Gut-related issue (NSAID damage, leaky-gut symptoms, IBD-adjacent
inflammation)?
→ Oral BPC-157 250–500 mcg twice daily for the gut-specific effect. Subcutaneous BPC won’t cover this case. - Surface wound or skin-level injury?
→ Topical GHK-Cu first-line. The injectable healing pair is overkill for purely cutaneous concerns. - Scheduled surgery (orthopedic, sports-injury reconstruction,
abdominal procedure)?
→ Different protocol shape - pre-op set-up window, anesthesia wash-out, post-op timing of BPC + TB after wound closure, plus the GHK-Cu scar-minimisation branch. See Peptides Around Surgery.
Representative stacks
Stack 1 - Localized tendon (e.g. patellar, Achilles)
- BPC-157 250 mcg subcutaneous twice daily, near the site, weeks 1–6
- TB-500 5 mg per week (split Mon/Thu), weeks 1–4 loading
- TB-500 2.5 mg per week, weeks 5–8 maintenance
- Progressive loading rehab in parallel; the peptides shorten the curve, they don’t replace the work
Stack 2 - Multi-site / older user / aggressive timeline
- BPC-157 500 mcg subcutaneous once daily, weeks 1–12
- TB-500 5 mg per week loading, weeks 1–6; 2.5 mg/week maintenance, weeks 7–12
- Mod GRF 100 mcg + Ipamorelin 200 mcg pre-bed, weeks 1–12
- Bloodwork: IGF-1 baseline + 6 weeks; HbA1c baseline + 12 weeks (see Bloodwork for Peptide Users)
Stack 3 - Gut + soft-tissue overlap
- Oral BPC-157 250 mcg twice daily, weeks 1–6 (gut effect)
- Subcutaneous BPC-157 250 mcg twice daily near the injury site, weeks 1–6 (joint/tendon effect)
- TB-500 systemic load if the soft-tissue component is significant
- The two BPC routes don’t cross-replace - oral hits the gut, injectable hits the joint. Both are needed if both targets are.
What stops people
- Cost reality. A real 8-week stack of BPC + TB-500 + GH axis is $300–$600 in research-chemical pricing depending on dosing. Vendors at half that are typically a quality problem, not a deal - see Sourcing and Verification.
- Skipping the rehab. The peptides accelerate healing of whatever tissue is being formed at the injury site. Without progressive loading, that tissue is scar, not aligned collagen. The peptide cycle ends, the scar fails under load, and the user blames the peptide.
- Underdosing. Online “100 mcg BPC daily” protocols underperform because they’re extrapolated from rodent dosing without scaling. The 250–500 mcg twice-daily range is what produces user-reported results.
- Reconstitution mistakes. Lyophilized BPC-157 in a 5 mg vial reconstituted with 2 mL gives 2.5 mg/mL = 250 mcg per 0.1 mL. Confirm the math before drawing; see Syringe-Draw Dosage Math.
- Active malignancy. Both BPC-157 (VEGF) and TB-500 (angiogenesis) are relative contraindications in active cancer contexts. The mechanisms are general pro-growth; that’s the right tool for healing and the wrong tool for tumor suppression. Get screened first if you’re in a high-risk window.
Monitoring on this protocol
- Functional outcomes > subjective ones. ROM, pain on loading, return-to-load milestones, single-leg or single-arm tests - track these weekly. “Feels better” is not a data point.
- Bloodwork: see Bloodwork for Peptide Users. The healing pair itself doesn’t move bloodwork meaningfully, but adding the GH-axis stack does - track IGF-1, fasting glucose, HbA1c.
- Photographic documentation for visible swelling or surface healing. Day-zero photo plus weekly is enough to make progress legible across a 6-week cycle.
- Reassess at week 4. If there’s no functional improvement in a pure soft-tissue injury after 4 weeks of the default pair, something is wrong - diagnosis, dosing, source quality, or rehab program. Don’t add more peptides into a non-responding cycle; investigate why first.