Two years of clean dosing, then the same patch of stomach starts to feel rubbery, the injection volumes start to absorb unevenly, and the next few cycles produce inexplicably weaker bloodwork on the same protocol. That’s lipohypertrophy - the slow scarring of subcutaneous tissue from repeated injections in too small a zone - and it’s the most common avoidable failure mode in long-term peptide use.
This article lays out the safe SC sites, what lipohypertrophy actually feels like before it’s visible, the basic infection-prevention checklist, and rotation grids for the three most common cadences (daily, BID, weekly).
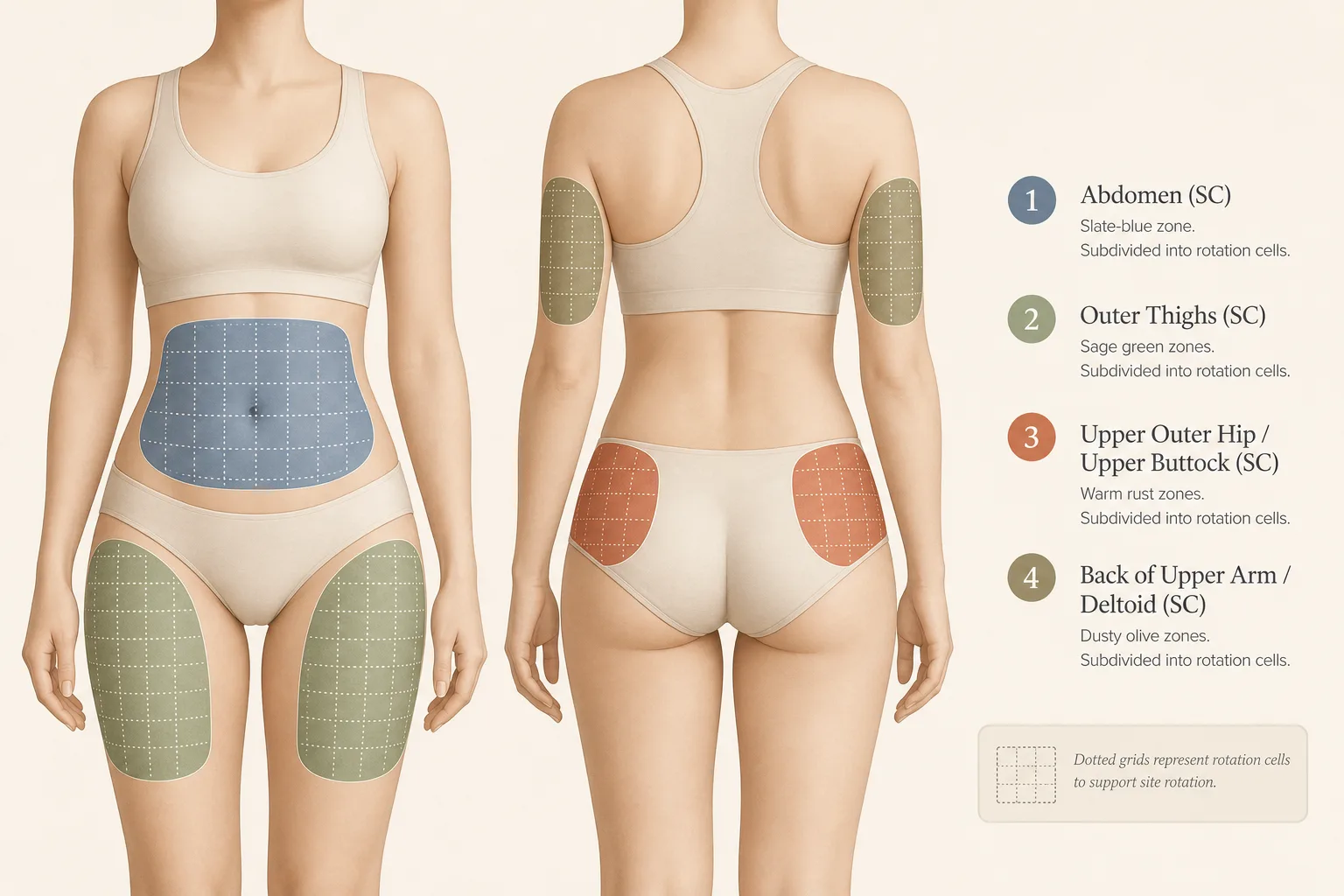
The four SC zones, in order of preference
Almost every peptide on this site is dosed subcutaneously. The four anatomically safe SC zones, in roughly the order most operators reach for them:
- Abdomen. The default zone. A roughly hand-width band running horizontally across the midsection, two finger-widths away from the navel in every direction. Generous tissue depth, easy to pinch, fastest absorption of the four zones.
- Outer thigh. The lateral surface of the upper thigh, palm-sized region halfway between hip and knee. Slower absorption than abdomen, very forgiving for daily use because the area is large.
- Upper buttock / outer hip. Upper outer quadrant of the buttock, above the gluteal fold. Often overlooked. Forgiving tissue, slower absorption profile, ideal for compounds where slower distribution is fine (most GH secretagogues, BPC-157 systemic).
- Upper outer arm (deltoid SC). The fatty pad on the back of the upper arm. Smallest of the four zones. Fine for occasional use; not enough surface area to handle daily or BID protocols on its own.
All four zones tolerate the small-gauge insulin needles (29G–31G, 5–8 mm) used for almost all peptide work. None of them tolerate being stabbed in the same square centimetre repeatedly for months - that’s the whole point of the rotation grid below.
Lipohypertrophy: what it is, what it feels like, what to do
- What it is. Localised proliferation of subcutaneous fat and fibrous tissue caused by repeated insertion in the same area. Pharmacology of the tissue changes: absorption gets slower, more variable, and sometimes unpredictably fast when needle placement happens to find a less-scarred patch nearby. The practical effect is dose-response drift on a stable protocol.
- What it feels like before it’s visible. Pinch the tissue where you usually inject. Healthy SC tissue feels uniformly soft and gives easily. Early lipohypertrophy feels firmer, slightly rubbery, sometimes nodular - like a thin layer of clay just under normal fat. By the time it’s a visible bump or a hardened patch you can see in profile, it’s well established.
- How to check. Once a month, palpate every site you’ve been using. Do it at the same time of day in similar conditions. Compare to a site you’ve never injected (under the bra line, behind the knee). Drift is detectable months before it becomes visually obvious.
- What to do if you find it. Stop injecting that area for at least 8–12 weeks. Move to a fresh zone. Light massage, warm compresses, standard tissue-recovery measures help; the actual mechanism is just not-injecting-here. Mild lipohypertrophy reverses in a few months. Severe, long-standing cases sometimes leave permanent fibrotic patches.
Infection prevention: the actually-load-bearing parts
Real infection rates from clean SC peptide injection are very low - well below what you’d see for IM injections, blood draws, or any procedure with deeper tissue exposure. But the rare cases that do happen are almost always a violation of one of these:
- Wash hands before drawing. Soap and water for 20 seconds. Hand-sanitiser is acceptable if you have nothing else; soap is better.
- Alcohol-swab the vial stopper before each draw. Wipe, then let it air-dry - a wet stopper drags alcohol into the vial which is counter-productive on most peptide stabilities.
- Alcohol-swab the injection site before insertion. Same air-dry rule. Inject through clean, dry skin.
- One needle, one injection. Don’t reuse insulin syringes. The cost saving is trivial, the dulling of the needle dramatically increases tissue trauma, and a reused needle that’s touched skin once is no longer sterile for the next draw.
- Don’t inject through clothing. Looks fast and clinical in movies; in real life it drags fibres through the puncture.
- Don’t inject through visibly inflamed, broken, or rashed skin. Pick a different site that day.
- Recon water hygiene matters. Use bacteriostatic water, not sterile water alone, for any reconstituted peptide that will be used over multiple days. The benzyl alcohol preservative buys you the multi-day window. See Reconstitution Fundamentals.
What does not meaningfully change infection rates: brand of alcohol swab, brand of needle, the difference between povidone-iodine and 70% isopropyl, gloves vs no gloves for the user (though gloves are sensible if there’s any wound on the injecting hand). Don’t over-engineer this; do the actual basics consistently.
Rotation grids by cadence
The simple principle: don’t inject within ~2 cm of a previous spot for at least 7–14 days, and don’t inject the same broad zone twice in a row. The grids below operationalise that for the three most common cadences. Day-by-day version with zone-cell pairs and the cell-numbering convention in the Injection Rotation Grid cheat sheet.
Daily (e.g. Tesamorelin, low-dose Semaglutide on tighter cadence, BPC-157)
Two-week rotation across the four zones. Subdivide each zone into 7 cells of roughly 2 cm spacing.
| Day | Zone | Cell |
|---|---|---|
| 1, 8 | Abdomen left | Cells 1, 4 (rotate within zone) |
| 2, 9 | Abdomen right | Cells 1, 4 |
| 3, 10 | Outer thigh left | Cells 1, 4 |
| 4, 11 | Outer thigh right | Cells 1, 4 |
| 5, 12 | Upper outer hip left | Cell 1, 4 |
| 6, 13 | Upper outer hip right | Cell 1, 4 |
| 7, 14 | Upper outer arm (alternate sides each occurrence) | Cell 1, 4 |
This pattern revisits each zone roughly every 7 days, and within a zone a specific cell gets revisited every ~14 days - well within the tissue’s recovery window.
BID (e.g. Ipamorelin + Mod GRF stacks, BPC-157 high-frequency healing protocols)
Two injections per day means you exhaust a zone faster. Strategy: pair zones by time of day so each zone still gets revisited only on a 7-day cadence.
- AM: Day 1 abdomen-left → Day 2 outer-thigh-left → Day 3 upper-hip-left → Day 4 upper-arm-left → cycle right-side → cycle back.
- PM: Day 1 abdomen-right → Day 2 outer-thigh-right → same pattern, mirrored.
- Within each zone-day, choose a cell at least 2 cm from the previous occurrence in that cell. A small body-map sticker on the bathroom mirror with a date marker is the low-tech tool that actually works.
Weekly (e.g. Semaglutide, Tirzepatide, CJC-1295 (DAC))
Weekly cadence is the easiest case. Even a four-cell rotation gives each spot a full month of recovery between injections. The risk pattern is different though:
- Pen-injectors land in roughly the same spot. Dialled-pen GLP-1 devices encourage habit-injection in one stomach quadrant. Force a four-zone monthly rotation regardless.
- Larger volumes. Some weekly compounds use 0.5–1 mL volumes that produce visible fluid pockets. Pinching a generous skinfold and going perpendicular to the surface helps; massaging after injection doesn’t.
- Suggested rotation: Week 1 abdomen-left → Week 2 outer-thigh-left → Week 3 abdomen-right → Week 4 outer-thigh-right → repeat. Avoid arms for high-volume weekly compounds.
Special cases
- Local injection for tendon repair. Some users front-load BPC-157 injections close to a healing tendon for the first 2–4 weeks. The rotation principle still applies - rotate within a 6–8 cm radius around the target site rather than insisting on the standard four-zone grid - but don’t inject the same square centimetre twice in a week even when treating the same injury.
- AAS users co-running peptides. Don’t share zones between SC peptide work and oil-based IM AAS injections. The IM zones (glute, quad, ventro- gluteal, deltoid IM) are deeper and structurally different. The deltoid IM location overlaps with the SC arm zone - pick one or the other for that arm, not both.
- Injection-site discomfort that doesn’t resolve. A bruise is normal. Tenderness for 24–48 hours is normal. Pain that sharpens at day 3 or worsens with motion, redness expanding past the immediate injection site, fever of any kind - that’s a clinical visit, not a forum post.
- Cold compounds. Some users inject straight from the fridge. Cold peptide stings more and produces more local irritation. Letting the syringe sit at room temperature for 5–10 minutes before injection is a small quality-of-life improvement at no cost to stability.
What stops people
- Picking a favourite zone. Almost everyone has a preferred abdominal quadrant they reach for unconsciously. That’s how lipohypertrophy starts. The grid above only works if you commit to following it on the days you don’t feel like rotating.
- Skipping the monthly palpation. Tissue drift is silent until it’s not. Five minutes once a month catches it months earlier than waiting for a visible bump.
- Reusing needles. The single most common operator mistake. Doesn’t directly cause infections often, but does increase tissue trauma significantly - which compounds the lipohypertrophy problem.
- Injecting into already-traumatised areas. A bruise is the signal that the tissue is recovering. Going back to that exact spot before it has healed is how scarring accelerates.
- Confusing fast absorption with bad rotation. If a usually-slow compound suddenly hits hard, that’s rotation working - you found a well-perfused fresh patch. Not a problem to fix; a signal to keep rotating.
Cross-references
- Reconstitution Fundamentals - bacteriostatic water, sterile technique on the vial side.
- Syringe, Draw and Dosage Math - needle gauge selection and volume math.
- Storage and Handling Best Practices - cold-chain hygiene that complements site hygiene.
- Cycling Strategies - cadence decisions that determine which rotation grid you need.