“Cycling” is one of those words that sounds like it means one thing and actually means three. When someone says “you have to cycle that”, they could be referring to any of:
- Receptor desensitisation - the receptor itself stops responding when stimulated continuously, so you have to give it a break to recover sensitivity. This is a real, measurable, dose-of-time-matters problem.
- Theoretical-risk washout - the compound has a mechanism (angiogenesis, growth-factor signalling) that’s great in the short term and poorly understood over years of continuous exposure. Cycling here is risk hygiene, not pharmacology.
- Titrate-and-hold dose strategy - not really a cycle at all. It’s a way to find the lowest effective dose and stop there. Treating it as a cycle (climb the dose, drop, climb again) is the wrong mental model and produces worse outcomes.
These three need different protocols. This article maps the major peptide classes onto the right one.
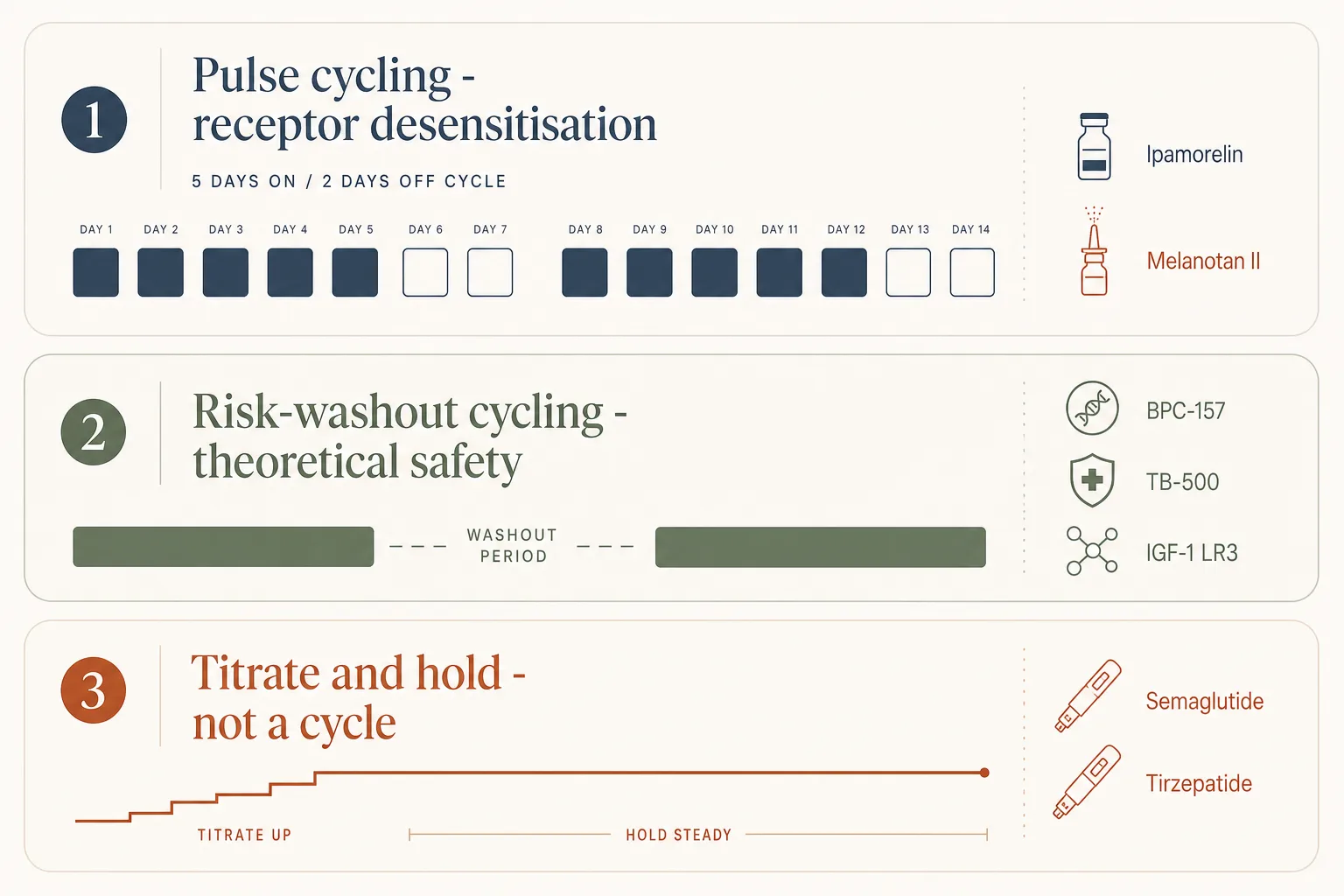
1. Receptor desensitisation - pulse to keep the door open
This is the textbook case for cycling. A receptor stimulated continuously downregulates: surface expression drops, intracellular coupling weakens, the same dose delivers a smaller signal. Pulsing - periods on, periods off - lets the receptor recover.
GH secretagogues (GHRH + GHRP)
- The compounds: Ipamorelin, Mod GRF 1-29, CJC-1295 (DAC), sermorelin, tesamorelin.
- The mechanism: ghrelin and GHRH receptors on the pituitary desensitise under continuous occupancy. CJC-1295 with DAC is the worst offender by design - the DAC modification keeps it bound for days, which raises baseline IGF-1 but blunts the natural pulse.
- The standard pattern: 5 days on, 2 days off, indefinitely. Some operators run 8 weeks on, 4 weeks off on top of that for a longer macro-cycle when bloodwork shows IGF-1 plateauing despite the same dose.
- Practical decision: Mod GRF + Ipamorelin pre-bed only is forgiving and many operators run it close to continuously without measurable downregulation. Multi-pulse protocols (BID/TID with CJC) need the 5/2 pattern to keep working.
Melanocortin agonists
- The compounds: Melanotan II, Melanotan I, PT-141.
- The mechanism: the relevant receptors (MC1R for tanning, MC4R for libido and appetite) tachyphylax fast. MT-II in particular has a clean loading-then-maintenance pattern: aggressive daily dosing to saturate, then weekly maintenance once the pigment is in.
- The standard pattern:
- MT-II tanning: 100 mcg ramp → 250 mcg → 500 mcg/day until target shade (1–3 weeks), then 500 mcg–1 mg once weekly as maintenance. Pigment persists for months.
- PT-141 libido: on-demand dosing only, never continuous. Receptor saturation happens fast and the compound stops working if used daily.
- Practical decision: these are not “run a 12-week cycle” compounds. They’re pulse-on-purpose compounds. Treating MT-II like a daily multivitamin produces a tan plateau in week three and a darker pigment in moles than in skin.
2. Theoretical-risk washout - cycle for risk hygiene, not pharmacology
Some peptides keep working continuously but raise downstream risk concerns over long exposure. Cycling here is conservative risk management. The mechanism doesn’t require the break; the long-tail safety story does.
Angiogenic / repair peptides
- The compounds: BPC-157, TB-500, GHK-Cu (systemic).
- The concern: BPC-157 acts in part through VEGF-mediated angiogenesis. New blood vessel growth is the point during a tendon repair; it is also a theoretical risk amplifier for any pre-existing malignancy. Long-term human safety data is thin.
- The standard pattern: 4–8 weeks on, then a washout of at least the same length before resuming. Some operators bracket cycles around bloodwork (CBC, basic tumour-marker screen) when running them often.
- Practical decision: there is no pharmacokinetic reason these stop working at week 8. The cycling is about not stacking continuous angiogenic signalling on top of years. Run focused healing cycles, document what you treat, take the break when the joint stops hurting. See Bloodwork for Peptide Users for the monitoring panel.
IGF-1 family direct agonists
- The compounds: IGF-1 LR3, IGF-1-DES, PEG-MGF.
- The concern: direct IGF-1 elevation, especially at LR3 levels that bypass binding-protein regulation, is the strongest growth-factor signal in the catalogue. The cancer-risk story for IGF-1 specifically is more concrete than for BPC/TB - epidemiology shows higher IGF-1 in adulthood is associated with several cancers.
- The standard pattern: 4-week cycles, equal-length washout, with annual breaks. Most experienced users front-load IGF-1 LR3 in the first half of an AAS cycle and discontinue, rather than running it continuously.
- Practical decision: the cycling discipline here matters more than in the angiogenic class because the risk model is more concrete. Skip cycles unless body-comp goals demand them.
3. Titrate-and-hold - not a cycle, a dose strategy
The biggest mental-model error around modern fat-loss peptides is treating GLP-1 as a cycle. It isn’t. The dose strategy is: titrate up to the lowest dose that produces steady fat loss, hold there, and only climb when the deficit has stalled for at least two weeks.
- The compounds: Semaglutide, Tirzepatide, Retatrutide, oral GLP-1s.
- What “cycling” would mean: climb the dose, ride it, drop the dose, ride it back up. People do this. It mostly produces nausea on the re-ramp and lost ground on the drop.
- What actually works:
- Climb the dose every 6–8 weeks, not every 4. The package insert is the floor.
- Stop climbing the moment fat loss is steady at 0.5–1% body weight per week.
- When the goal is reached, taper to a maintenance dose (often half the cutting dose) for 6–12 months, then re-evaluate.
- Discontinuation requires a maintenance protocol (calories, protein, training) from week one of cutting, not week one of stopping.
- Why this matters for body comp: rapid up-and-down dose curves correlate with worse muscle preservation outcomes. See GLP-1 and Muscle Preservation.
4. Compounds that are usually fine continuous
Not everything cycles. A few classes work continuously without measurable downregulation or a strong long-term risk story:
- Tesamorelin - clinical protocols for HIV-lipodystrophy run daily for 26+ weeks. The pulsatile architecture of GHRH agonists protects the receptor better than DAC-modified compounds do.
- GHK-Cu topical - daily skincare use is the protocol. Continuous low-dose topical exposure has not produced concerning signals.
- Thymosin Alpha-1 - immune-modulator with chronic-use clinical history; cycling is not the default.
- Selank, Semax - ramp dosing, then run continuously through a project or stress window.
5. Reading a protocol critically
Three questions to ask whenever someone’s cycling advice doesn’t match a source:
- Which mechanism is the cycle for? If it’s receptor desensitisation, the on/off lengths should match the receptor’s recovery time (days to weeks). If it’s risk hygiene, the cycle length is essentially a judgement call about cumulative exposure (months). If it’s neither, it’s probably wrong.
- Is bloodwork driving the cycle? A 5/2 pattern based on tachyphylaxis is structural; an 8-on/4-off macro-cycle should be triggered by IGF-1 plateauing or by hematocrit climbing, not by the calendar.
- Does the discontinuation plan exist? “Run for 12 weeks and stop” is incomplete. The post-stop maintenance protocol - for GLP-1, for GH axis, for MT-II - is what determines whether the cycle was worth running.
What stops people
- Cycling for the wrong reason. The 4-on/4-off pattern that’s correct for BPC-157 produces nothing useful when applied to MT-II. The mechanisms are different.
- Treating GLP-1 as a cycle. See above. The dose-up, dose-down, dose-up rhythm wastes potential lean-mass preservation.
- Skipping the washout because the compound is “clean.” Clean side-effect profile in week 1 is not the same as clean cumulative exposure over 18 months. BPC-157 is the obvious example.
- Stacking three desensitising compounds without staggering. Running CJC-DAC + Ipamorelin + extra Mod GRF on the same 5/2 pattern is more receptor strain than the pattern was designed for. Stagger or simplify.
- No bloodwork bracketing. Cycling decisions get a lot easier with IGF-1, hematocrit, fasting glucose, HbA1c, and lipids on a timeline. See Bloodwork for Peptide Users.
Cross-references
- GH Axis Playbook - pulsatile vs DAC decision in detail.
- Semaglutide vs Tirzepatide vs Retatrutide - per-compound titration nuance.
- GLP-1 and Muscle Preservation - why the titrate-and-hold dose strategy matters for body comp.
- Bloodwork for Peptide Users - the cadence that turns cycling decisions from calendar-driven into data-driven.
- When a Peptide Cycle Fails - the diagnostic to run if the cycle isn't producing the response the bioassay or sentinel said to expect.
- Injury Recovery application - BPC/TB stacking and the standard healing-cycle bracketing.
- Peptide Stacks That Compound Risk - the catalog of combinations where the cycling discipline this article describes is the structural answer to the risk-compounding problem.