“Melanocortins” sound like one thing. They’re actually a family of peptides - alpha-MSH, beta-MSH, gamma-MSH, ACTH - binding five different G-protein-coupled receptors with five different jobs. Most of the confusion around Melanotan I, Melanotan II, and PT-141 dissolves once you map each compound to the receptor it actually binds. This article does that map and ends in a decision tree.
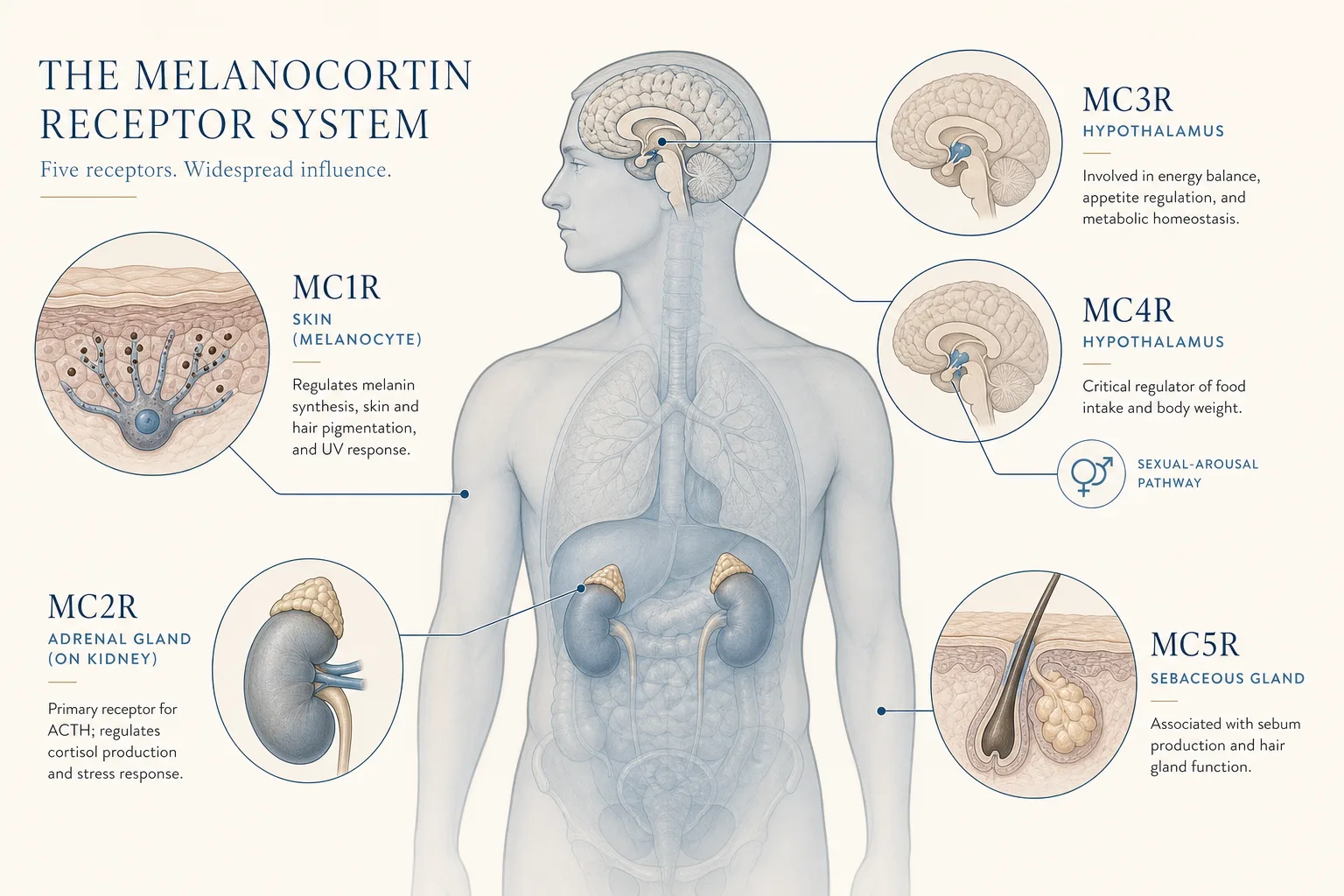
The five receptors
- MC1R - expressed on melanocytes in the skin. Binding it switches melanin synthesis from pheomelanin (red/yellow) to eumelanin (brown/black). This is the tanning receptor. Genetic loss-of-function is the “ginger” phenotype: low eumelanin, high UV sensitivity.
- MC2R - expressed on the adrenal cortex, binds ACTH, drives cortisol release. None of the cosmetic / libido peptides target this one. Out of scope here.
- MC3R - expressed in the hypothalamus and limbic system. Modulates energy homeostasis and inflammation; less studied than MC4R but shares some functional space.
- MC4R - the one that does most of the interesting work. Hypothalamic; gates appetite (loss-of-function MC4R is a known monogenic obesity cause) and central sexual arousal pathways. The receptor responsible for both PT-141’s libido effect and a chunk of MT-II’s side-effect profile.
- MC5R - sebaceous glands and exocrine tissue. Linked to sebum production and possibly thermoregulation. Not the target of any of the compounds in scope, but worth knowing because broadband agonists touch it.
All five receptors are active. The endogenous ligand alpha-MSH binds MC1R, MC3R, MC4R, and MC5R with similar affinity - meaning “just give people MSH” would produce every effect at once: tan, appetite drop, libido shift, sebum bump. That’s why receptor selectivity is the whole story for the synthetic compounds.
The compounds, mapped to receptors
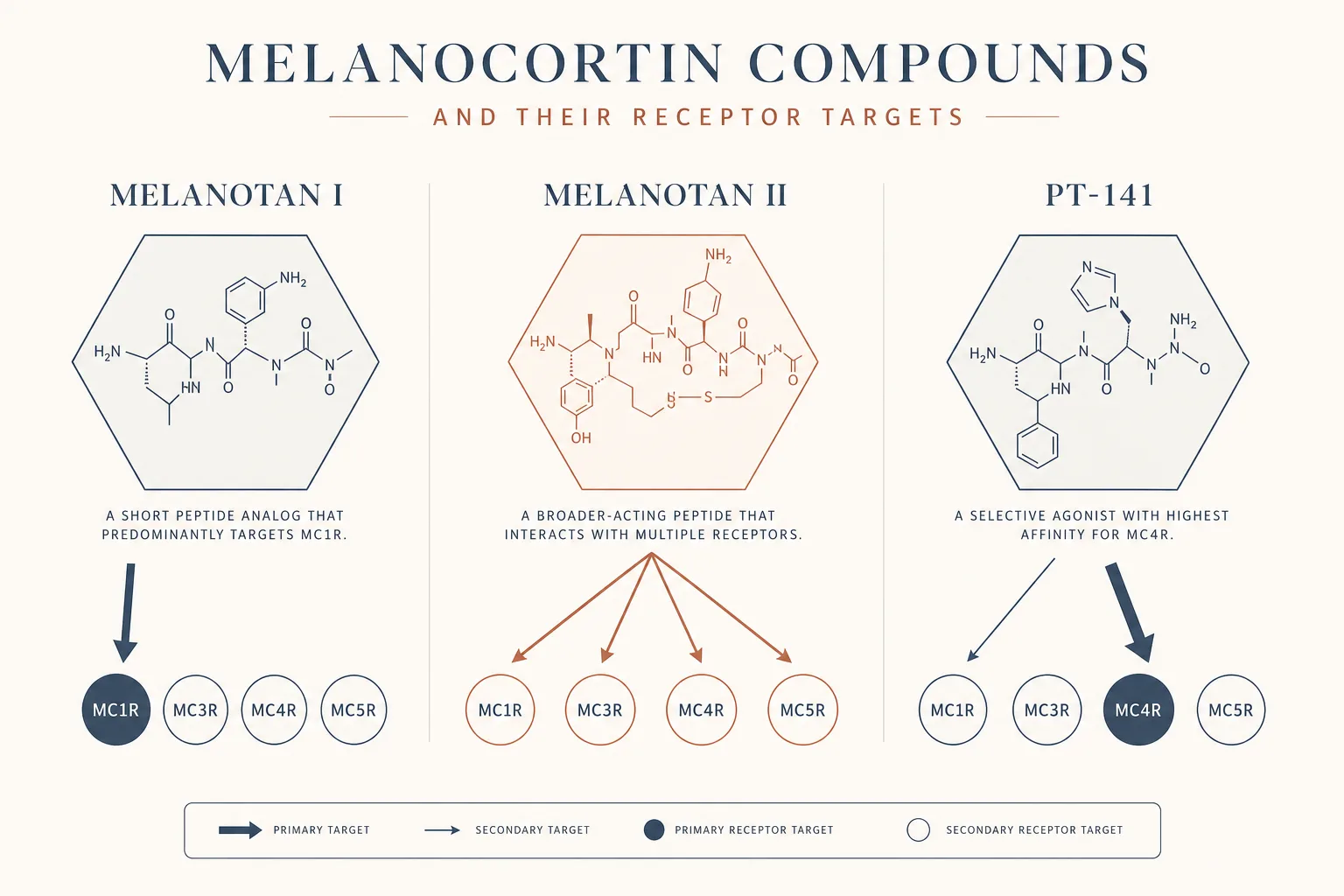
Melanotan I (Afamelanotide)
- Receptor profile: Strong preference for MC1R; substantially less affinity for MC3R/MC4R/MC5R. Closer to a “skin-only” molecule than its cousin.
- Half-life / form: The free peptide has a short serum half-life; delivered as a sustained-release subcutaneous implant (Scenesse), it covers months per dose. Injected free-peptide grey-market preparations require frequent dosing.
- Effect: Eumelanin synthesis without the central side effects (nausea, flushing, libido shift) of MT-II. Gives the tan; doesn’t give the rest.
- Regulatory: FDA- and EMA-approved as Scenesse for erythropoietic protoporphyria (a UV-photosensitivity disorder). Cosmetic use is off-label.
- Who it’s for: Anyone whose goal is tanning or photoprotection only, who wants the cleanest mechanism and is willing to accept the slower onset and higher cost of the clinical product (or the hassle of frequent injection if going grey-market).
Melanotan II
- Receptor profile: Broad agonist. Binds MC1R (tanning), MC3R, MC4R (libido / appetite), and MC5R. This is why it does “everything” the alpha-MSH family does, and why the side-effect surface is wider than MT-I.
- Half-life: ~1 hour (free peptide), with biological effects on pigmentation lasting much longer because the downstream eumelanin response is cumulative.
- Effects: Tan (MC1R), erections / libido increase (MC4R), appetite suppression (MC3R/MC4R), facial flushing and transient blood pressure changes (mixed), nausea (MC4R), darkening of moles and freckles (MC1R, broadly across all melanocytes including ones you don’t want darker).
- Regulatory: Not approved. Research chemical with FDA warning letters on file.
- Who it’s for: Users who explicitly want the multi-effect package - tan plus libido plus appetite suppression - and are willing to accept the side-effect breadth and the lack of a clinical product. The skin-survey requirement (see below) is more important here than for any other compound on the page.
PT-141 (Bremelanotide)
- Receptor profile: Selectivity tilted toward MC4R, with measurable activity at MC1R and MC3R but the central libido effect is MC4R-driven. Cleaner than MT-II for the “sexual desire only” use case.
- Half-life: ~2 hours. Used acutely (45–90 minutes before sexual activity), not as a daily protocol.
- Effects: Increased sexual desire and arousal, central rather than vascular - this is the key differentiator vs PDE5 inhibitors like sildenafil. Side effects: nausea (MC4R), facial flushing, transient BP rise, occasional headache. Some users get mild skin pigmentation effects from off-target MC1R binding, especially with frequent use.
- Regulatory: FDA-approved as Vyleesi for acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women. Off-label use is broad in both sexes.
- Who it’s for: Anyone who wants a libido / desire effect through a central pathway, not a vascular one. Particularly relevant when PDE5 inhibitors fail or are contraindicated, or when the actual issue is desire rather than mechanics. Stacks with PDE5 inhibitors when both desire and vascular limits are present, but the BP interaction needs respect. Full protocol, the BP-baseline pre-screening, the PDE5-priapism stacking caveat, and the central-vs-vascular decision tree live in the Libido and Arousal application.
Setmelanotide (briefly)
Imcivree (setmelanotide) is the MC4R-selective agonist approved for monogenic obesity (POMC, PCSK1, LEPR loss-of-function). It’s outside the cosmetic / libido scope of this article but worth knowing exists, because it’s the cleanest proof that MC4R-selective agonism is a tractable drug-development target. Anyone with a confirmed genetic indication should be on the approved drug, not on a research-chemical alternative.
Side effects, mapped
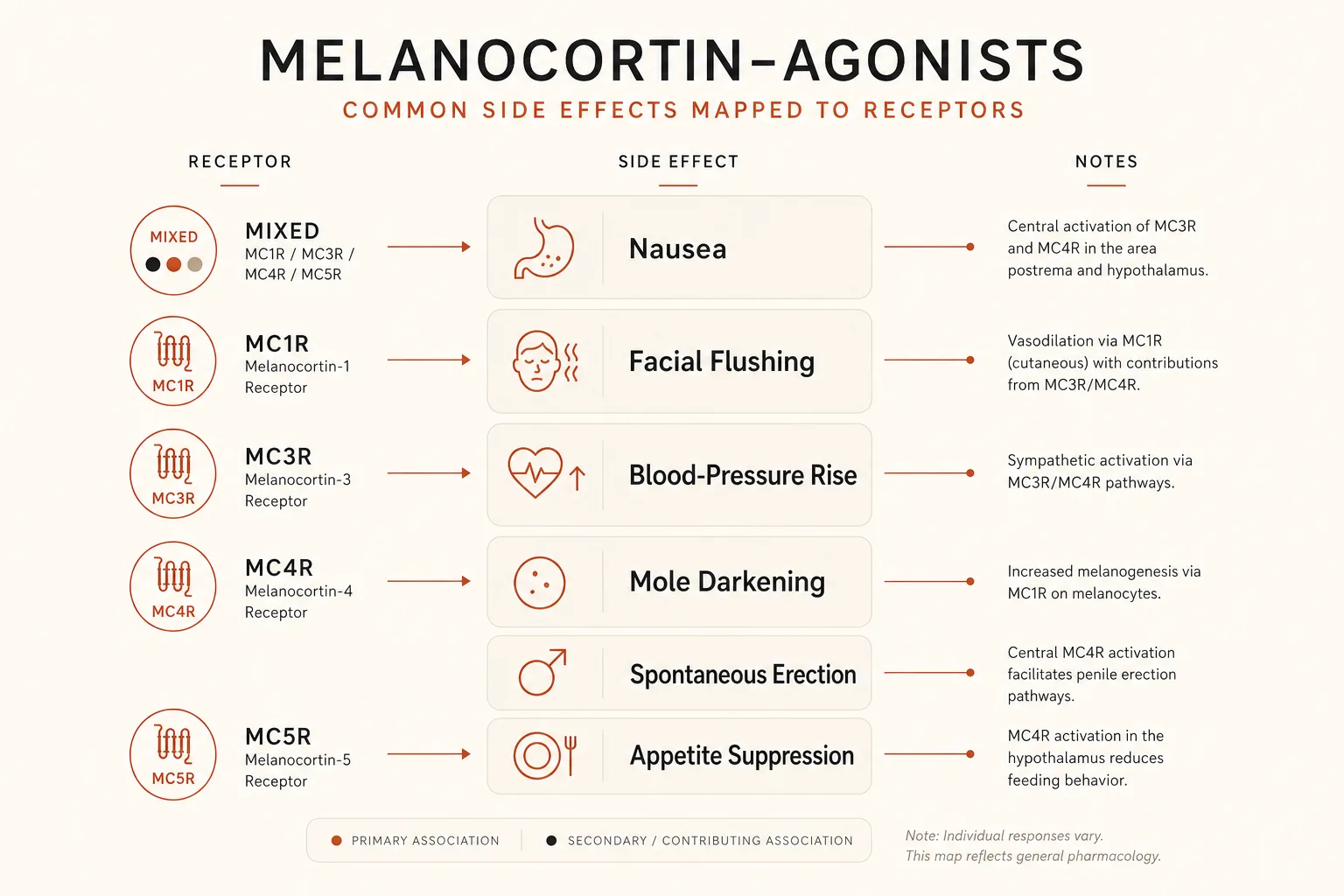
Most of the side effects of MT-II and PT-141 are predictable from the receptor map:
- Nausea - primarily MC4R. Worse with MT-II (broad agonism) than PT-141 (more selective). Tolerance often develops over a few doses.
- Facial flushing - mixed mechanism; MC1R contributes via skin vascular effects, MC4R via central autonomic outflow. Common, transient, harmless.
- Transient blood pressure increase - central MC4R-driven sympathetic outflow. Largely why uncontrolled hypertension is a contraindication for PT-141 (and a reason for caution on MT-II).
- Mole darkening, freckle darkening, new pigmented spots - MC1R on all melanocytes, including ones you didn’t intend to activate. Document existing nevi photographically before any MT-II protocol.
- Spontaneous erections - MC4R. Expected with MT-II at higher doses; less with PT-141 at typical doses but possible.
- Appetite suppression - MC3R/MC4R. A wanted effect for some MT-II users, an unwanted effect for others. Not typically clinically significant on PT-141’s acute dosing pattern.
Decision tree
- Is the only goal tanning or photoprotection?
→ Melanotan I. Cleanest receptor profile for that single goal. Use the implant if accessible; the injectable form requires more frequent dosing. - Is the goal sexual desire / libido, with no interest in tanning or appetite
effects?
→ PT-141. MC4R-selective, FDA-approved channel available. Acute dosing only. - Is the goal both tanning and libido, and is appetite suppression a feature
rather than a bug?
→ Melanotan II. Accept the broader side-effect surface. Document moles before starting. - Is there uncontrolled hypertension, melanoma history, or a high density of
atypical nevi?
→ Stay out of the broad melanocortin agonists. PT-141 is conditional (BP), MT-II is contraindicated (pigmentation), MT-I is the safest of the three for the pigmentation-history case but skin oncology should be looped in regardless. - Is the issue actually mechanical (vascular) rather than central?
→ PDE5 inhibitor (sildenafil, tadalafil), not a melanocortin compound. PT-141 is the wrong tool for a vascular problem.
Practical notes
- Loading vs maintenance for MT-II: The standard pattern is a loading phase (250–500 mcg/day until target pigmentation, plus moderated UV exposure because melanocyte stimulation needs UV to fully express), followed by maintenance dosing once or twice a week. Going faster usually trades nausea for no real time saved. The day-by-day ramp, antihistamine timing, and the dermatology baseline as a separate runbook in the MT-II Loading Protocol guide.
- Acute dosing for PT-141: 1.25–1.75 mg subcutaneous, 45–90 minutes before activity. The Vyleesi auto-injector is at 1.75 mg. Higher doses don’t improve the desired effect and load the side-effect curve.
- UV is still required for the cosmetic-tanning effect of either MT-I or MT-II. The peptides predispose melanocytes to make eumelanin; the UV signal is what triggers the actual response. “Tan in a vial, no sun” is marketing, not biology.
- Bloodwork: Resting BP weekly during any active protocol is the minimum. See Bloodwork for Peptide Users for the full panel.
What this article doesn’t cover
ACTH analogs (cosyntropin, tetracosactide) are out of scope here - they target MC2R for adrenal stimulation, not the cosmetic / libido axis. AGRP and the inverse-agonist pharmacology being explored for cachexia are research-stage. The MC1R-selective full-agonist class beyond afamelanotide (vusolimogene, novel candidates) is moving but none of those are realistic options today.