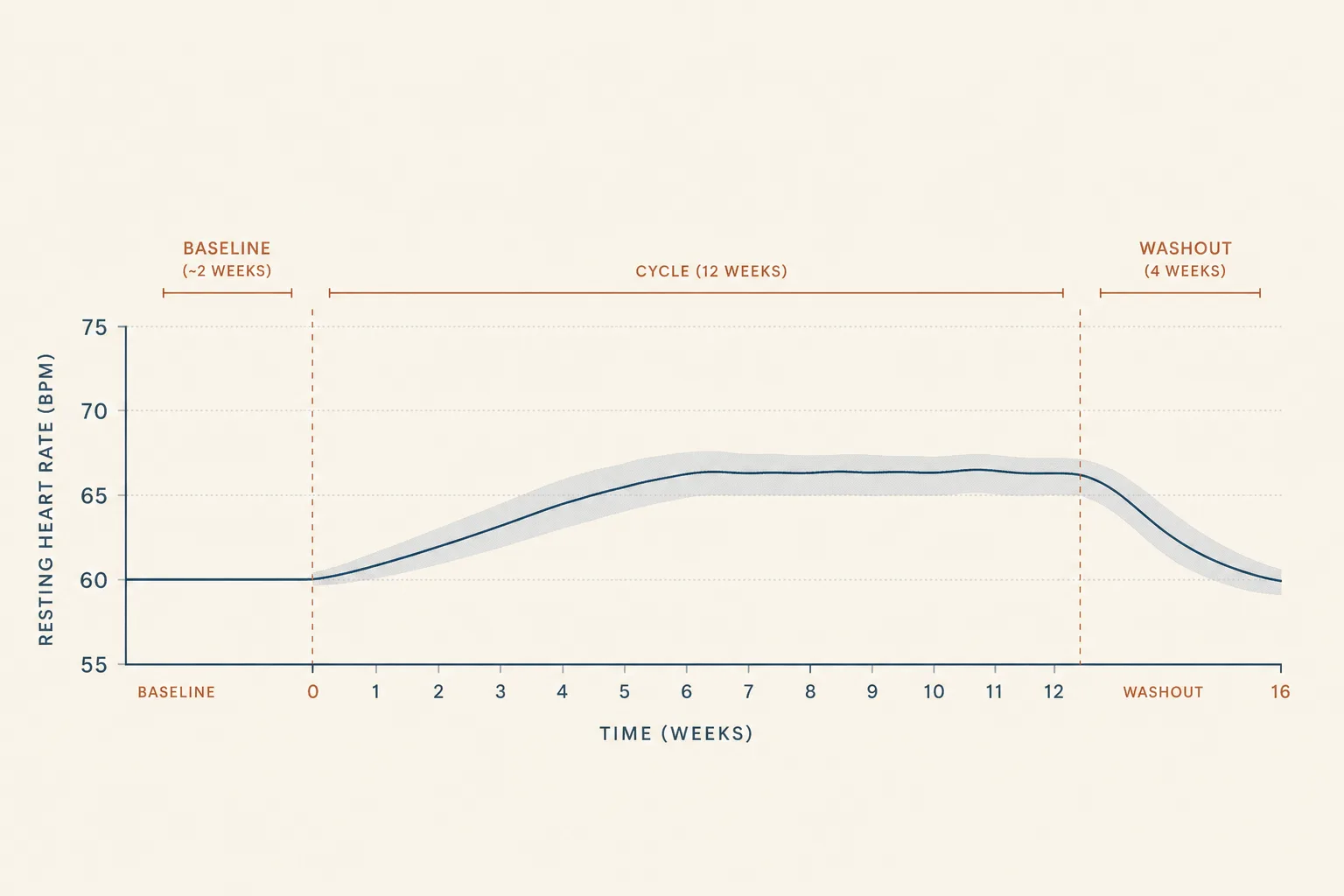
Resting heart rate moves on most peptide cycles that touch metabolism, autonomic tone, or fluid balance. The signal is small enough that point measurements miss it, scattered enough across the catalog that no single article covers it, and reliable enough that a 14-day trend is one of the cheapest sentinels available. This article puts the per-class numbers in one place, sets the discipline for daily measurement, and draws the line between "expected drift" and "stop the protocol."
Why heart rate moves at all
Three mechanisms account for almost everything you'll see in this catalog:
- Glucagon-receptor activity. Activation raises energy expenditure and produces a measurable elevation in resting heart rate. Retatrutide is the clearest example; survodutide and other glucagon-active dual / triple agonists carry similar signatures.
- Central autonomic outflow via MC4R. The melanocortin-4 receptor sits in hypothalamic circuits that gate sympathetic tone. Activate it acutely (PT-141, MT-II loading doses) and you get a transient blood pressure and heart rate response. Chronic MC4R agonism shifts the baseline upward.
- Fluid retention. Continuous-elevation GHRH stacks (CJC-1295 DAC) and exogenous HGH at bodybuilding doses produce real water retention. The plasma-volume expansion increases stroke-volume demand and pushes resting heart rate up a few beats per minute. Reverses on washout.
Beat-to-beat variability (HRV) tracks something subtler - the parasympathetic / sympathetic balance - and is a useful complement for users who already have a wearable that captures it. The resting heart rate number is the cheap version; HRV is the deeper version of the same physiological story.
Per-class baseline expectations
| Compound | Expected RHR drift on protocol | Mechanism | Reverses? |
|---|---|---|---|
| Semaglutide (high-dose obesity protocol) | +1–3 bpm | Mild central + indirect (weight loss can lower it the other way) | Yes, on washout |
| Tirzepatide (15 mg) | +3–5 bpm | GIP/GLP-1 dual agonism; partial weight-loss offset | Yes, on washout |
| Retatrutide (high-dose Phase 2 arms) | +5–8 bpm typical, individual outliers higher | Glucagon-receptor activation | Yes, on washout - but the trial population shows meaningful inter-individual variance, so anyone with cardiovascular sensitivity should watch the trend carefully |
| PT-141 (Vyleesi, on-demand) | Acute peak +5–10 bpm at 1–2 h, returns to baseline in hours | Central MC4R outflow | Per dose; no chronic shift at recommended frequency cap |
| MT-II (loading phase) | +2–5 bpm during loading; ~baseline on maintenance | Broad melanocortin agonism, autonomic | Yes, fades to baseline as melanocyte saturation hits |
| CJC-1295 (DAC), continuous | +2–4 bpm via fluid retention | GH continuous elevation → plasma-volume expansion | Yes, on washout (~2–3 weeks) |
| Somatropin (HGH) at body-comp doses | +2–4 bpm; higher with concurrent insulin | Water retention + cardiac workload | Yes, on washout (1–4 weeks) |
| Pulsatile GHRH + GHRP (Mod GRF + Ipamorelin) | None expected | - | - |
| BPC-157, TB-500, GHK-Cu | None | - | - |
| MOTS-c, KPV, thymosins | None expected | - | - |
These ranges come from the registration-trial readouts (SURMOUNT-1, Jastreboff 2023 retatrutide, SELECT for semaglutide, the Vyleesi label) and from accumulated bodybuilding-context observation for the GH compounds. Individual responses fall outside the typical band; the point of measuring is to know whether you're on the curve or off it.
The discipline that makes the sentinel useful
- Baseline before the cycle. Two weeks of daily morning measurements before starting a new protocol. Average, not single number - circadian and autonomic noise is real, a single morning can be 5 bpm off the running average.
- Same conditions every day. First minute after waking, before getting up, before checking phone. Caffeine, illness, alcohol, late workouts, and short sleep all push the number around. Note them next to the reading.
- Trend, not single days. A 7-day rolling average is the floor; 14-day is the more honest signal. A single +6 bpm morning is noise; a 7-day average drifting +6 bpm is the protocol talking.
- The protocol is the variable, not the only variable. Training load shifts, dieting state, sickness, and seasonal temperature shift the number too. Cross-check the trend against those, not just against the protocol's calendar.
HRV: the deeper signal
Heart rate variability - the millisecond-level differences between consecutive beats - tracks parasympathetic tone better than mean resting heart rate. On peptide cycles, HRV drops a few percent alongside the RHR rise on glucagon-active and continuous-GH compounds; it stays mostly flat on pulsatile GHRH + GHRP and on the BPC / TB / GHK family.
- Useful when you already have it. Apple Watch, Oura, Whoop, Garmin - HRV measurement is a commodity now. If your wearable provides a 7-day-average HRV number, track it alongside RHR. Don't buy a new device just to add this layer.
- Bigger drops are the signal worth paying attention to. A 10–15% sustained HRV drop on a glucagon-active compound, alongside a +5 bpm RHR drift, is a stronger combined signal than either number alone.
- Confounders are bigger than for RHR. HRV moves on alcohol, late meals, training day vs rest day, illness - anything that shifts autonomic tone. The trend over 14+ days is the only signal worth reading.
What turns drift into a stop signal
- Sustained >10 bpm rise vs baseline. Outside the typical band even for retatrutide. Pause the protocol, retest baseline conditions, rule out sickness or short sleep. If it persists, the dose is too high or the compound isn't tolerable for this user.
- RHR rise paired with palpitations, chest pressure, or new exertional symptoms. Not negotiable. Stop the protocol and get a clinical workup. Strict-liability framing: the protocol is the simplest variable to remove.
- Resting BP pattern shift alongside the RHR rise. Sustained >10 mmHg systolic shift with the RHR climbing means the autonomic load is not where it should be. Same pause-and-evaluate response.
- HRV crash >25% sustained over 14 days. Bigger than typical training-stress drops. Look at whether something else (training overload, illness, sleep debt) is confounding before blaming the peptide; if peptide is the likeliest variable, dose down or pause.
- RHR steady but exercise capacity dropping. Subtler signal - same morning RHR but harder to hit usual workout intensities. Sometimes early in glucagon-active protocols, often resolves with adaptation; track for 2 weeks before deciding.
What the sentinel doesn't catch
- Arrhythmia in real time. Resting heart rate misses paroxysmal events. If a wearable can do single-lead ECG (Apple Watch, KardiaMobile), occasional rhythm strips are a cheap addition for users on glucagon-active compounds.
- Vascular stiffness changes. Long-term HGH or DAC use can stiffen large arteries - the RHR sentinel doesn't detect this. A pulse-wave-velocity or carotid-IMT measurement at a clinic, every couple of years for sustained users, catches what wearables miss.
- Acute hypotension on PT-141 or MT-II. The peak BP rise is usually what gets discussed, but some users get the opposite - a transient drop, especially when stacked with a PDE5 inhibitor. RHR rises to compensate; the underlying BP drop is what matters and isn't visible on a wrist sensor.
- Bunk peptide. If a compound that should drift your RHR (retatrutide, tirzepatide) doesn't move it at all over 8 weeks of titration, that's a sourcing question, not a tolerability win. See Sourcing and Verification.
Common cautions
- Don't read single days. The single-day noise floor is roughly ±5 bpm even on a stable baseline. Trends, not points.
- Caffeine confound is bigger than people remember. A morning coffee before measurement adds 2–4 bpm. If you can't move the measurement to before coffee, at least keep the coffee timing constant across the cycle.
- Training load matters. A new resistance training programme can drop RHR by 3–5 bpm over 4 weeks independently of any peptide. Hard to attribute drift if both variables changed at once.
- Illness flag, not panic. A respiratory infection can spike RHR by 10+ bpm for a week. Note it, don't discontinue.
- The wearable error budget. Wrist sensors are accurate within ~3 bpm at rest; chest straps and dedicated pulse oximeters are tighter. The cheap consumer device is good enough for trend-tracking; just stick with one device.
Cross-references
- Peptides and Insulin - the metabolic counterpart to this article. Heart rate is the cardiac sentinel; HOMA-IR and CGM are the metabolic ones.
- Bloodwork for Peptide Users - the lab-side panel discussion that the wearable sentinels here complement.
- Semaglutide vs Tirzepatide vs Retatrutide - the source of the per-compound RHR expectations table above.
- CagriSema and the Pipeline Past Retatrutide - heart-rate signature is where the glucagon-active branch of that pipeline reads distinctly from the GLP-1 / GIP branch.
- Libido and Arousal application - the pre-screen for PT-141 / MT-II that includes baseline BP and HR.
- Peptides for Endurance Athletes - the audience whose RHR baseline sits 10-15 bpm lower than the population mean and where the drift signals in this article have to be tracked off the user's own baseline rather than against population norms.
- Peptides and Blood Pressure - the BP companion to this piece. Different mechanisms, different per-class directions, same daily- measurement discipline. Read both for the full cardiovascular sentinel frame.
What this article doesn't cover
Specific cardiology investigations - echocardiogram, stress test, Holter monitor - are clinic-level studies and out of scope. The decision to obtain those is downstream of a sustained drift the sentinel above caught. Sport-context heart-rate-zone training is a different topic with its own literature; resting heart rate as a health sentinel and training-zone heart rate are not the same question. AAS-context heart-rate considerations (LVH, blood pressure under cycle load) are adjacent and deserve their own treatment.