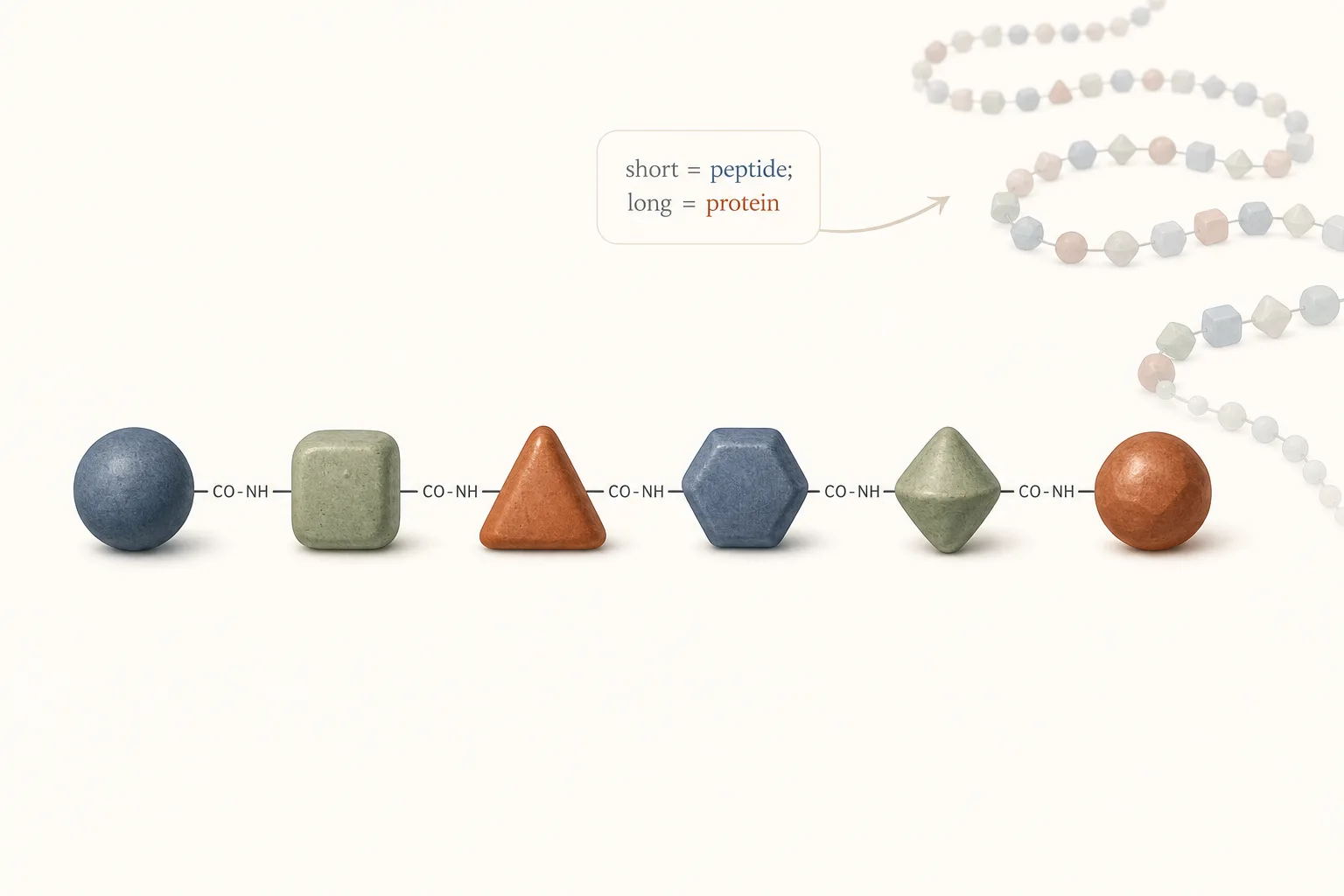
What is a peptide?
Peptides are short chains of amino acids - same chemistry as proteins, just shorter. The convention is fuzzy: anything under about 50 amino acids is a peptide, longer than that gets called a protein. In biology, many peptides act as signalling molecules - hormones, growth factors, neurotransmitters, immune signals. In medicine and research, some peptides become drug ingredients (insulin, semaglutide, somatropin, GLP-1 analogues generally). Many others remain experimental with limited human evidence, which is the territory most of this catalogue covers.
Why peptides matter to a body-hacker audience
The audience this site is written for already knows the steroid / GLP-1 / SARM landscape. Where peptides fit in that landscape is what this article is mostly about. Three honest framings:
- Less risky end of the spectrum. Most peptides in this catalogue have lower acute-toxicity profiles than AAS, lower chronic-disease drift than supraphysiologic AAS use, and shorter biological footprints than long-acting drugs. They're not risk-free, but the risk frame is different.
- Mechanism-of-action literature usually exists. "Less tested than ibuprofen" is a reasonable mental model - animal data, in-vitro data, often early-phase human work. "Mystery chemical" is wrong. The exceptions are flagged.
- Practical decisions favour modesty. The peptide class is mostly subtle effects on top of a working foundation (sleep, training, diet). Stack expectations accordingly. The catalogue's content-plan is honest about which compounds are speculative.
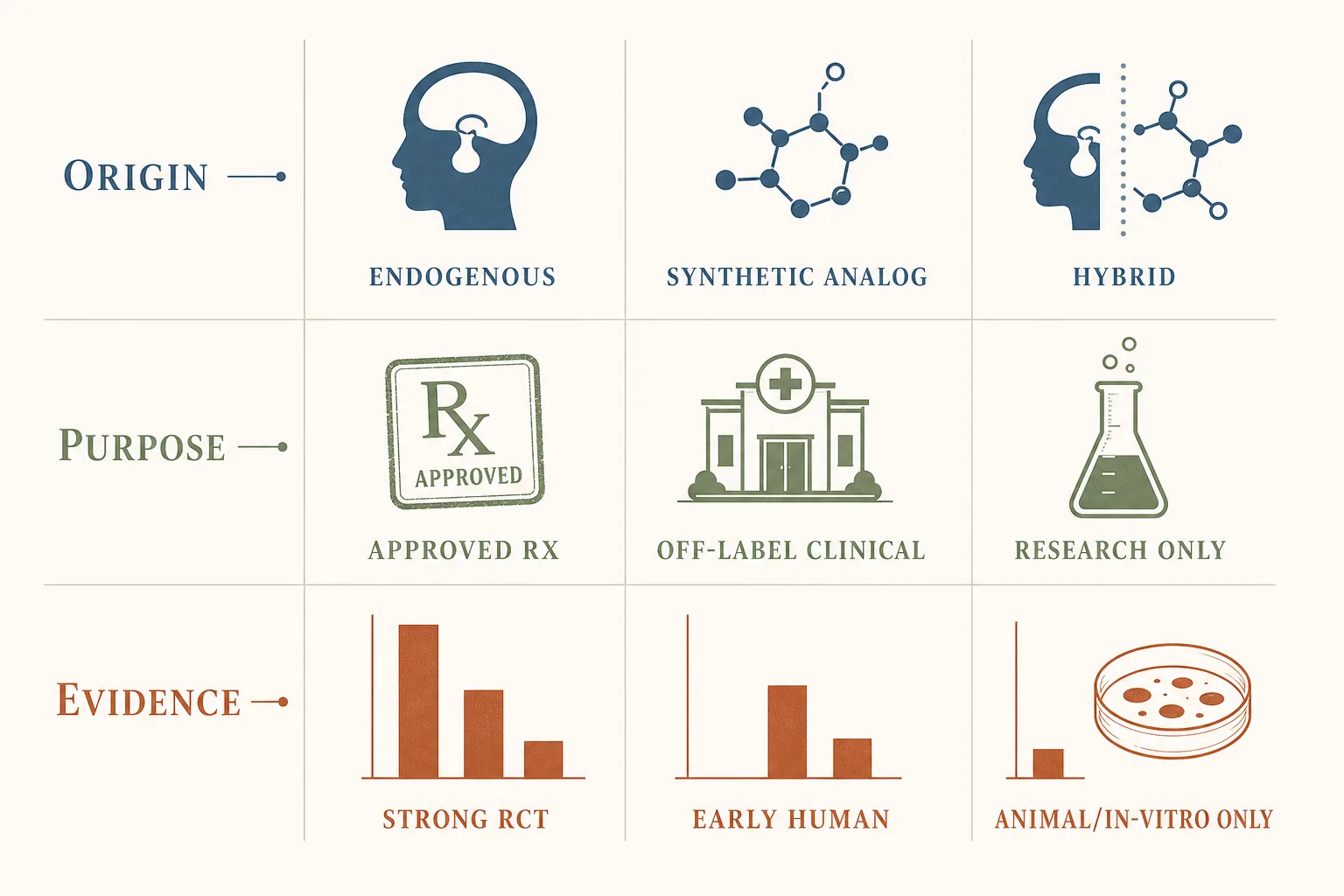
A useful way to classify peptides
- By origin: endogenous (naturally occurring in the body) vs. synthetic analogues. BPC-157 is endogenous in spirit (a fragment of a human stomach protein); semaglutide is a synthetic analogue of GLP-1.
- By purpose: approved therapeutic use, off-label clinical use, or research-only interest. Liraglutide and tirzepatide are FDA-approved drugs; PEG-MGF and IGF-1 LR3 are research-chemical territory.
- By evidence level: strong randomised human trial data, early human data, animal-only, or in-vitro only. The evidence-tier label on each peptide page maps directly to this.
- By route: SC (subcutaneous, the default), IM (site-specific or higher-volume), oral (BPC-157 for gut, KPV), intranasal (Selank, Semax), topical (GHK-Cu). See Routes of Administration for the full breakdown.
What's in this catalogue
Nine canonical peptide classes covering the body-hacker space, plus a handful of compounds that don't fit a single class cleanly. The fastest survey of the territory is the Peptide Class Lookup; the short version:
- GH-axis (GHRH analogues + GHRPs): Mod GRF 1-29, Sermorelin, CJC-1295, Tesamorelin, Ipamorelin, plus recombinant HGH (Somatropin) at the systemic-replacement end. The pulsatile pre-bed Mod GRF + Ipamorelin stack is the canonical entry point.
- GLP-1 family: Semaglutide, Tirzepatide, Retatrutide, Liraglutide. The fat-loss class. Approved as Wegovy / Zepbound / Saxenda; "compounded" grey-market versions also widely available.
- Healing peptides: BPC-157, TB-500 (and full-length Thymosin Beta-4). The injury-recovery and joint-support core.
- Growth factors: IGF-1 LR3, IGF-1 DES, PEG-MGF, Follistatin-344. Bodybuilding hypertrophy class - also where the cumulative-cancer-exposure conversation lives.
- Melanocortin agonists: Melanotan II, Melanotan I, PT-141. Tanning, libido, sometimes both at once.
- Thymic peptides: Thymosin Alpha-1 (immune tone), Thymosin Beta-4 (repair, listed under healing peptides above).
- Russian nootropic peptides: Selank, Semax. Approved drugs in Russia for anxiety / cognitive impairment; research-chemical status in the West.
- Mitochondrial-derived peptides: MOTS-c, Humanin. Speculative-tier longevity space.
- Misc. AOD-9604, Fragment 176-191 (HGH lipolytic fragments), KPV (gut anti-inflammatory), Dihexa (cognitive plasticity), DSIP / Epitalon (sleep / circadian), LL-37 (antimicrobial, higher-risk).
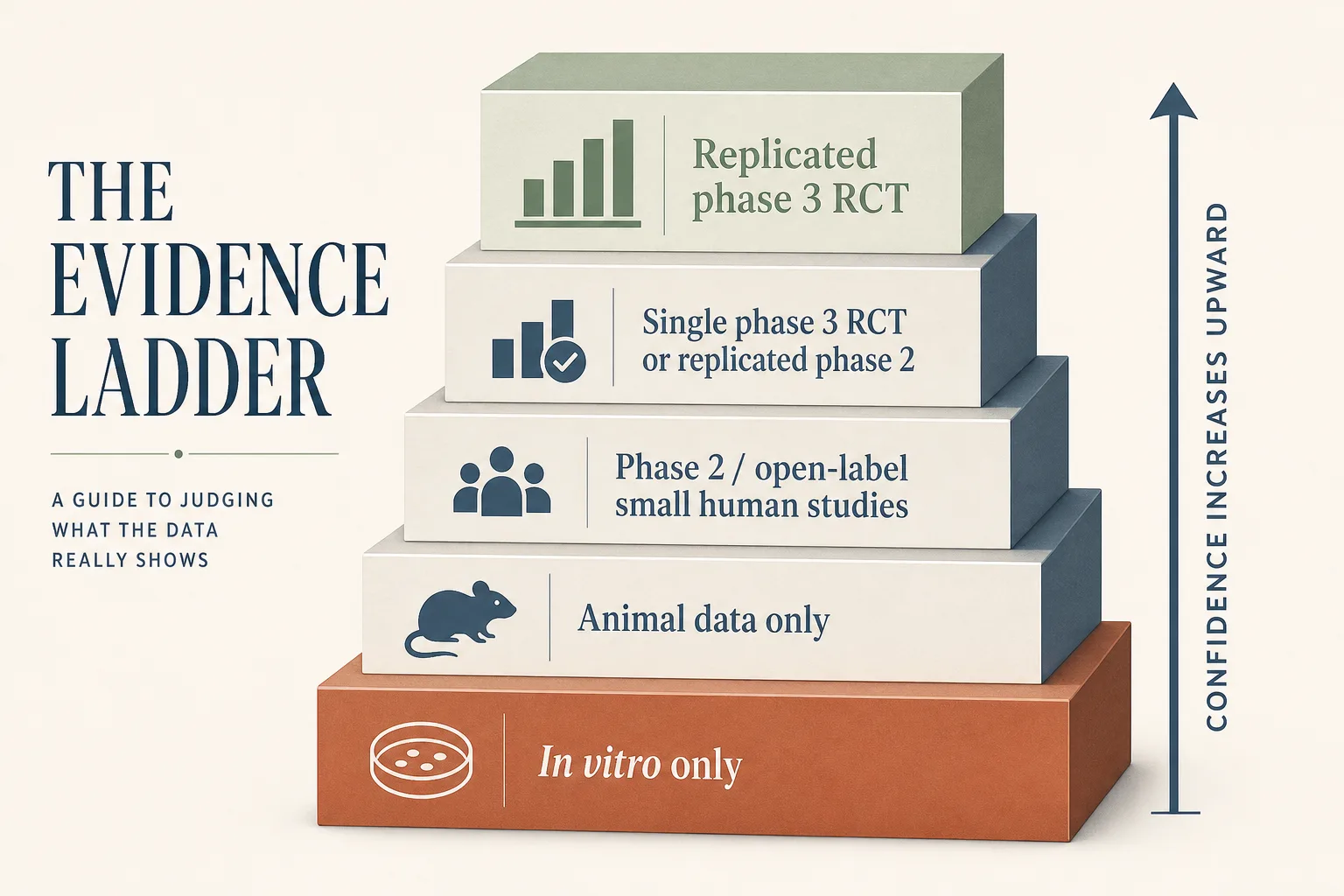
Evidence quality: what beginners should prioritise
- Human outcomes first. Prioritise well-designed human clinical trials over anecdote. SURMOUNT-1 (tirzepatide for obesity) is hard data; "I felt great on this peptide on Reddit" is weak data. Both can be true; only one carries weight in a decision.
- Look for replication. One positive small study is a signal, not a conclusion. The catalogue's evidence-tier labels weight this - "Limited data" means the human evidence base is small or unreplicated; "Clinical" means there's substantial replicated work.
- Check endpoints. Biomarkers can be interesting, but clinical outcomes matter more. IGF-1 going up on a GH-axis protocol is expected; whether body composition or recovery actually improved is the meaningful question.
- Assess uncertainty. Wide confidence intervals and short follow-up limit confidence. Animal-data extrapolation to humans is uncertain by default; species-specific receptor differences and dose-response curves don't translate cleanly.
Safety framing (honest, not preachy)
- Unknown purity and contamination risk are real. Non-regulated supply chains mean the contents of a given vial may not match the label. The catalogue tracks evidence rating per peptide but assumes nothing about your specific vendor. See Sourcing and Verification.
- Injectables carry extra risk. Contamination bypasses skin and gut barriers when you inject. Aseptic technique, cold-chain, single-puncture discipline - these aren't optional. See Storage and Handling Best Practices.
- "Natural" or "research peptide" labels prove nothing. A label is marketing copy. Independent third-party testing is the only objective signal of vial-content quality.
- If an effect claim sounds dramatic and source quality is weak, treat it as unverified. "Adds 20 lbs of muscle in 8 weeks" claims usually trace back to AAS-stack contexts where the peptide isn't doing the work. Skim for the unstated co-factors.
- The catalogue has one global risk note, not per-page disclaimers. The site treats the audience as adults already in this space. Don't expect the disclaimer-sprinkling pattern of consumer-facing health blogs; it's not the editorial frame.
Red flags when reading peptide claims
- Only testimonials, no cited human trials or even animal trials.
- Claims of "no side effects" or "works for everyone." Real biology has variance; absolute claims signal sloppy thinking or marketing copy.
- No clear concentration, storage, or quality-control information.
- Confusing unit labels (mg vs mcg vs mL) without transparent math. See Syringe, Draw and Dosage Math for what the math should look like.
- Pricing structure that incentivises selling more peptides over answering questions accurately.
- Recommendations that don't differentiate routes (SC vs oral vs intranasal) when the route is part of the protocol - that's a signal the writer hasn't thought about route-bioavailability differences.
Beginner checklist before trusting any protocol
- Can you find a primary source (paper, guideline, label) for the core claim?
- Is the evidence mainly human, animal, or cell-only?
- Are risks, contraindications, and uncertainties explicitly discussed?
- Are calculations and concentration assumptions clearly shown?
- Does the protocol respect cycling (on/off) discipline, or is it "run continuously" framing?
- Are bloodwork-monitoring recommendations specific (which markers, what cadence) or vague?
The first protocol most readers consider
Pre-bed Mod GRF 1-29 + Ipamorelin is the standard entry point - a pulsatile GH-axis stack with the lowest-risk profile in the injectable-peptide space and a well-characterised evidence base. If you're new to the catalogue and want a single starting reference, the Pre-Bed GH-Secretagogue Protocol is the runbook, paired with the GH Axis Playbook for the why.
Other common starting goals route to different applications:
- Fat loss → Fat Loss application + GLP-1 Comparison.
- Acute injury → Injury Recovery; chronic joint pain → Joint Support.
- Sleep / recovery → Sleep and Recovery (Mod GRF + Ipa pre-bed is also the load-bearing protocol here).
- Skin / hair → Skin and Hair (topical GHK-Cu is the canonical case).
- Anxiety / cognitive focus → Anxiety and Calm / Cognitive Focus (Selank / Semax intranasal).
Where to go next
- Your First Peptide Cycle - the cycle-planning piece that pairs with this one: pick one goal, set up supplies and baseline, run the protocol with a 4-week reassessment milestone.
- Peptide Class Lookup - the catalogue's nine canonical classes mapped to representative compounds and the applications where each shows up. The fastest survey of the territory.
- GH Axis Playbook - the deepest single-receptor-family writeup; reads cleanly even without prior context.
- GLP-1 Comparison - for the GLP-1 family (semaglutide / tirzepatide / retatrutide) which is the most-asked-about set in the catalogue.
- Fat Loss application - first goal-oriented application most readers reach for; shows how the article + peptide-page + guide pieces combine into a protocol.
- Sourcing and Verification - read this before buying anything in this catalogue.
- Coming Off: The Washout Window - what to expect when you stop a protocol; pairs with cycling-strategies.
- Peptides and Female Physiology - the small set of compounds and contexts where female-specific physiology is load-bearing on the decision (PCOS + GLP-1, PT-141 / Vyleesi label, MT-II demographics, pregnancy contraindications).
Sources
- FDA: Clinical Trials and Drug Development Process - https://www.fda.gov/patients/drug-development-process/step-3-clinical-research
- Oxford Centre for Evidence-Based Medicine (levels framework) - https://www.cebm.ox.ac.uk/resources/levels-of-evidence
- FDA: Unapproved drugs and patient harm - https://www.fda.gov/drugs/enforcement-activities-fda/unapproved-drugs-and-patient-harm