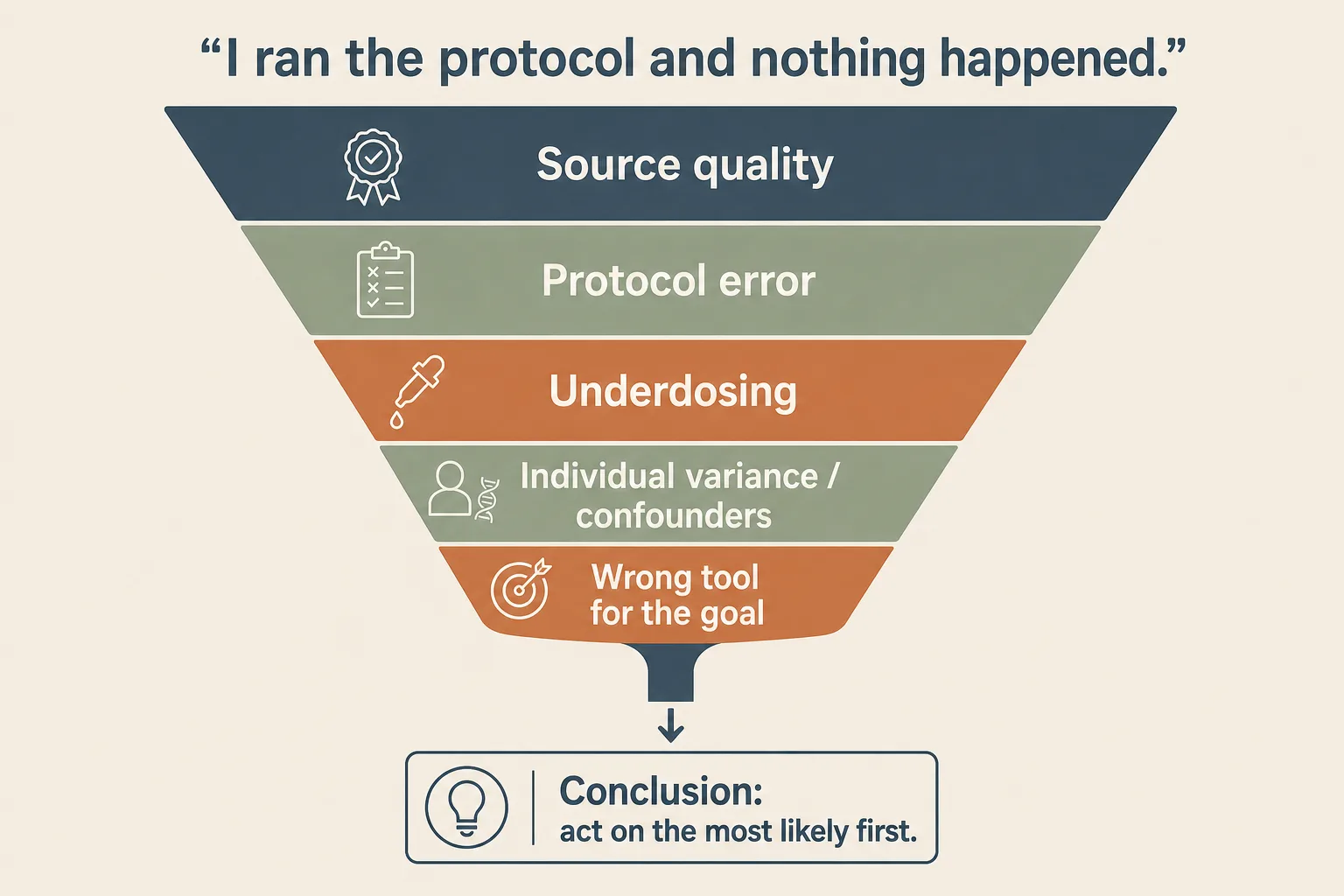
"I ran the protocol and nothing happened" is one of the most common things this audience says. It almost never means the peptide doesn't work in general; it usually means one of five things happened on this particular cycle, and the diagnostic order matters. Working through the list below before deciding the compound is bunk, the protocol is wrong, or your body is broken will save a surprising amount of money and frustration.
The five causes, in likelihood order
- Source quality. Most common. The vial contains a fraction of the labelled mass, the wrong peptide entirely, or a peptide that's been oxidised in shipping or storage. The response curve looks like nothing is happening because nothing is.
- Protocol error. The compound is real and at the right dose, but the timing, fasting state, route, or reconstitution math broke the protocol. Common with GH-axis stacks (food in the fasting window) and lipolytic fragments (insulin in the dosing window).
- Underdosing. The compound is real, the protocol is right, but the dose is below the response threshold for that user. More common at the cautious end of the dose range than people expect, especially for users scaling rodent dose recommendations down to "safer" human equivalents.
- Individual variance and baseline confounders. Some users are non-responders for biological reasons (receptor polymorphisms, concurrent medications, baseline hormone state). Less common than the first three but real. Confounders are things like sleep debt, training overload, dieting state, or illness that swamp the peptide signal.
- Wrong tool for the goal. The peptide does what it does; what it does isn't what you needed. PT-141 for an erection problem of vascular origin, BPC-157 for chronic tendinopathy that's a remodelling failure rather than a proliferation bottleneck, GHK-Cu for diffuse hair loss when the issue is androgenic. The cycle worked at the mechanism level; it didn't move your specific problem.
1. Source quality (start here every time)
Grey-market peptide quality varies wildly. The vial may contain a small fraction of the labelled mass; the wrong peptide entirely; a peptide that's been oxidised in shipping; or material that was fine on arrival but degraded under your storage. Source-quality problems are the single most common explanation for failed cycles and the easiest to verify if you're willing to spend the money.
- Send a vial to a third-party lab. HPLC and mass spec on a fresh vial from the same lot. The marginal cost is small relative to the cost of running an entire failed cycle. See Sourcing and Verification.
- Bioassay where one exists. IGF-1 bloodwork on a GH-axis cycle should move at 6 weeks; MT-II should produce flushing and pigmentation in the loading phase; GLP-1s should quiet food noise in the first week at meaningful doses. No bioassay signal is a strong source-quality flag.
- Check oxidation history. If the vial worked initially and stopped working later, oxidation of a sensitive residue (Met, Trp, Cys) is plausible. Reconstituted vials oxidise faster than lyophilised powder; rehearse cold-chain discipline. See Cold Chain Reality and Understanding Peptide Purity.
- Salt-form correction. A "5 mg" vial delivered as a TFA salt may contain 4.0-4.5 mg of free peptide. Your real dose math depends on which. If you're at the low end of a dose range and the vial is heavy on TFA, the effective dose is further below threshold than the label suggests.
2. Protocol error (next most common)
Protocol errors fall into a few stable patterns. Each compound class has its own most-frequent way users break the protocol:
- GH-axis stacks: food in the fasting window. Insulin from carbohydrate intake suppresses the GH pulse the GHRH analog is trying to trigger. Eating 30 minutes before the pre-bed Mod GRF + Ipamorelin shot burns a quarter to most of the protocol depending on meal composition. See Peptides and Insulin for the mechanism.
- Lipolytic fragments (AOD-9604, Frag 176-191): insulin in the dosing window. These compounds need a truly fasted state to produce their lipolytic effect. Coffee with cream, a protein shake, or any glucose-load within 30 minutes pre or post-dose blocks lipolysis. The compound is fine; the conditions are wrong.
- BPC-157 / TB-500: location and frequency. Local injection close to the injury site outperforms remote SC for BPC-157; TB-500 is more systemic and less location-sensitive. Daily dosing for full-length Tβ4 vs weekly bolus for the TB-500 fragment is a common mix-up.
- GLP-1 family: titration too fast. Users who crush appetite suppression hard early tend to lose more lean mass and tolerate the GI events worse. The slow ramp isn't timidity; it's part of the protocol. See GLP-1 and Muscle Preservation.
- Reconstitution math. A 5 mg vial reconstituted with 2 mL gives 2.5 mg/mL = 250 mcg per 0.1 mL. Confirm the math before drawing. See Syringe-Draw Dosage Math.
- Storage drift. A reconstituted vial left at room temperature for an afternoon, repeatedly pierced through a contaminated septum, or frozen and thawed accidentally is a different vial than the one you started with.
3. Underdosing
The third most common cause: the compound is real, the protocol is right, but the dose is below the response threshold for this user.
- Bodyweight scaling matters more for some classes than others. GH-axis secretagogues saturate at roughly 1 mcg/kg for Ipamorelin; doses below that produce a smaller-than-expected pulse. GLP-1s and tirzepatide have titration ceilings well above what cautious users start at; "didn't work" at 0.25 mg semaglutide weekly is below the therapeutic range.
- Online dose tables are sometimes scaled from rodents. Mouse and rat dose-mg/kg numbers don't port to humans 1:1 because of metabolic-rate scaling. Human equivalent doses are usually higher in absolute terms than the rodent table suggests when scaled body weight to body weight.
- Some compounds need a loading phase. MT-II pigmentation response, TB-500 cell-migration window, BPC + TB proliferation-phase synergy: front-loaded doses produce most of the effect. Trickle-dose protocols miss the timing.
4. Individual variance and baseline confounders
Less common than the top three but real. Some users are legitimate non-responders for biological reasons; others have baseline confounders that swamp the peptide signal.
- Receptor polymorphisms. MC4R and MC1R variants are well documented and affect melanocortin response. GHRH / ghrelin receptor sensitivity varies. Loss-of-function alleles are rare but real.
- Concurrent medications. Beta-blockers blunt the cardiac signal of glucagon-active compounds. Statins interact with some metabolic peptides indirectly. PPI use affects oral peptide absorption (KPV, oral BPC).
- Baseline state. Sleep debt, training overload, illness, or aggressive dieting can swamp a peptide's signal in either direction. A user running a hypertrophy stack on 4 hours of sleep nightly will see less response than the same protocol in a recovered state.
- Hormonal context. AAS use, TRT status, menstrual cycle phase, or perimenopausal hormone shifts change how downstream peptide effects register. The compound may be working; the system around it has a different baseline.
5. Wrong tool for the goal
The most embarrassing and often the most overlooked. The cycle worked at the mechanism level; the mechanism wasn't what you needed.
- PT-141 for vascular ED. PT-141 produces central arousal; if the issue is peripheral vascular, PDE5 inhibitors are the right tool. See Libido and Arousal.
- BPC-157 for chronic tendinopathy. The proliferation-phase repair mechanism BPC + TB hits is most relevant in acute injury. Chronic tendinopathy is partly a failed-remodelling problem; BPC + TB helps but doesn't fix the underlying loading issue. See BPC + TB synergy.
- GHK-Cu for hair loss that's androgenic. GHK-Cu helps follicle health and stress signalling; it doesn't block DHT. If the loss pattern is androgenic alopecia, finasteride / dutasteride is the right tool.
- GH-axis stack for fat loss when the deficit isn't there. The GH axis enhances lipolysis at the margin; it doesn't override caloric intake. A user running CJC + Ipamorelin in a calorie surplus and not losing fat isn't running a failed protocol; they're running a correct protocol on a stacked constraint.
The walkthrough you can actually run
- Pull a bioassay where possible. IGF-1 at 6 weeks for GH-axis. Body composition trend over 8 weeks for GLP-1. Pigmentation/flushing trajectory for MT-II. Subjective food noise for early GLP-1. If the bioassay didn't move, suspect source quality first.
- Audit the protocol against the standard. Did the fasting window hold? Was reconstitution math right? Did the dose match the protocol's middle, not bottom? Was cycle-frequency respected?
- Send a vial for HPLC + mass spec. Costs less than the cycle. If main peak is below 95%, identity doesn't confirm, or the salt form math hasn't been corrected for, you have your answer.
- Reassess the goal. Did the protocol target the actual mechanism your problem needs? If not, the cycle succeeded mechanistically and failed on goal-fit.
- Look at confounders. Sleep, training load, diet, illness, concurrent medication. If a major confounder is present, the next cycle without it answers the question more cleanly than retrying with the same context.
When to abandon the cycle vs persist
- Abandon if the bioassay is dead. A completely flat IGF-1 response on a GH-axis cycle, zero food- noise change on a meaningful GLP-1 dose, no pigmentation on MT-II at loading dose: source quality. Test the vial; replace or restart.
- Persist with adjustment if the protocol was the error. Most protocol errors can be fixed mid-cycle. Tighten the fasting window, fix the reconstitution math, recover the sleep deficit. Give the corrected protocol two to four weeks before judging it again.
- Persist with dose escalation if underdosing is likely. Step up to the middle of the dose range, hold for two weeks, then judge. If still nothing, you've ruled out underdosing as the cause.
- Abandon if the goal-fit is wrong. No amount of dose adjustment fixes the mechanism mismatch. Different compound, possibly a different application class.
- Three full cycles of the same compound producing nothing is enough data. If you've cleared sourcing and protocol on three separate cycles and still see no response, you're a non-responder for biological reasons. Move on; the compound isn't going to start working on cycle four.
What stops people
- Anchoring on "the peptide doesn't work" too early. The compound class is unlikely to be the problem in most failed cycles. The list above is in likelihood order for a reason.
- Skipping the vial test because it costs money. A failed cycle costs more than a vial test. Operators who run multiple compounds without testing any of them are over-paying for the verification problem.
- Re-running the same compound from the same source after a failed cycle. If sourcing was the cause, the second run fails the same way. Either test the vial or change the source.
- Diagnosing without a bioassay. Subjective sense of "did anything happen" is unreliable for a single cycle. Tracking IGF-1, body comp, RHR, or pigmentation gives a more honest readout. See Bloodwork for Peptide Users and Heart Rate as a Peptide Sentinel.
Cross-references
- Sourcing and Verification - the operator-level guide for the testing pass that's the first step of this diagnostic.
- Understanding Peptide Purity - decoder for what the COA actually tells you about the vial you tested.
- Bloodwork for Peptide Users - the per-class panel and what counts as a real bioassay signal.
- Syringe-Draw Dosage Math - the most common reconstitution and drawing errors that produce "doesn't work" cycles.
- Peptides and Insulin - the fasting-window mechanism the GH-axis protocol-error case depends on.
What this article doesn't cover
Specific vendor recommendations are out of scope (and would rotate faster than article publication can keep up with). Diagnosis of the underlying medical condition - whether your back pain is a disc issue or a soft-tissue one, whether your hair loss is androgenic or telogen-effluvium - is medical-workup territory and outside the scope here. Female-physiology-specific considerations (hormonal cycle interaction, PCOS context, perimenopausal hormone shifts) are covered in Peptides and Female Physiology.