Peptide protocols without bloodwork are guesswork. The compounds in this catalog modulate growth, metabolism, immunity, and cardiovascular tone - all of which leave a measurable signature in routine labs. Pulling a panel before a cycle, again at steady state, and a third time off-cycle gives a closed feedback loop that costs less than one month of most peptides. This article gives a working framework: a baseline panel that everyone runs, per-class follow-ups, when to draw, and what the numbers mean.
For the at-the-lab quick reference - markers, cadence per class, and the exact requisition wording to copy onto a self-pay order - see the Bloodwork Panel Cheat Sheet.
The baseline panel
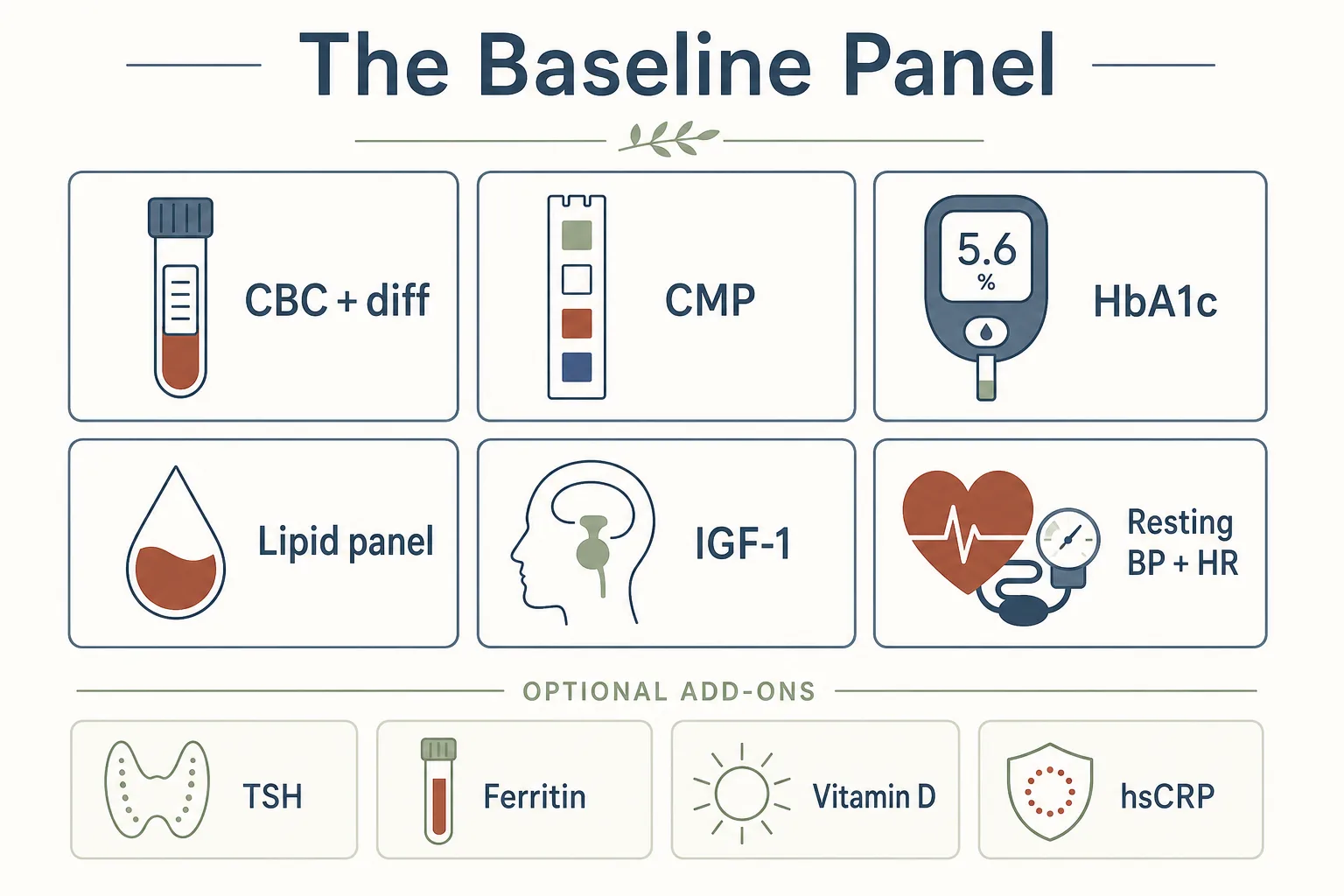
Before any cycle, regardless of compound, get the following. This is roughly a “CBC + CMP + lipids + HbA1c + IGF-1” package, plus a few extras worth tacking on once.
- CBC with differential - hemoglobin, hematocrit, white-cell differential, platelets. Catches anemia, polycythemia, and immune anomalies you wouldn’t have known about.
- Comprehensive metabolic panel (CMP) - fasting glucose, electrolytes, BUN/creatinine for kidney function, AST/ALT for liver, total protein, albumin.
- HbA1c - three-month glucose average. Anchor for anything in the GH axis or GLP-1 family.
- Lipid panel - total cholesterol, LDL, HDL, triglycerides. Important once GLP-1 or GH-axis compounds are involved.
- IGF-1 - the single most useful number for any GH-axis user. Even if you’re not running GH-axis peptides yet, a baseline matters because the question later is “moved how much from where.”
- Free and total testosterone, LH, FSH, estradiol (sensitive), SHBG - full hormone snapshot. Worth pulling once even on a non-androgen protocol; it contextualises body-composition changes.
- Resting blood pressure and resting heart rate - not blood, but cheaper than every lab and at least as informative for cardiovascular changes. Take both over a quiet week before starting.
Optional extras worth one-off baselines: TSH and free T4, ferritin, vitamin D 25-OH, hsCRP. Once you have these in your record they can be referenced for years; you don’t need to repeat them every cycle.
Per-class follow-up panels
GH axis (Mod GRF, CJC-1295, Ipamorelin, Tesamorelin, Somatropin)
- IGF-1 - the central readout. Confirms a compound is real and being absorbed; quantifies the response. For GHRH/GHRP stacks, expect modest movement; for CJC-1295 (DAC) and somatropin, expect the IGF-1 number to climb meaningfully.
- Fasting glucose and HbA1c - GH-axis activation drifts insulin sensitivity, especially with continuous (DAC) or supraphysiologic (somatropin) protocols. Glucose climbing into the high-90s fasting, or HbA1c moving from 5.2 to 5.7+, is the early signal.
- Lipids - usually neutral or slightly favorable on Tesamorelin; watch for triglyceride drift on high-dose somatropin.
- Prolactin (optional) - Ipamorelin at standard doses doesn’t move it meaningfully, but if you’re running an older GHRP (GHRP-2 or -6) it’s worth a check.
Timing: draw IGF-1 at least 8 hours after the last GHRH/GHRP injection (overnight fast is fine). For somatropin, draw at trough - the day of your next dose, before you inject.
GLP-1 family (Semaglutide, Tirzepatide, Retatrutide, Liraglutide)
- HbA1c, fasting glucose, fasting insulin - the metabolic readout. All three usually drop on incretin therapy.
- Lipid panel - expect favorable triglyceride and LDL changes as weight drops.
- CBC, CMP - kidney and liver markers; gallbladder events show as ALT/AST or alk-phos shifts.
- Resting heart rate - tracks tirzepatide and retatrutide more than semaglutide. Retatrutide’s glucagon-receptor activity is the reason heart rate is on this list; an upward drift of 5–10 bpm is expected, more than that warrants a dose re-think.
See also: Semaglutide vs Tirzepatide vs Retatrutide for the per-compound side-effect framing this panel is monitoring.
IGF-1 LR3 and other IGF-1 analogs
- Fasting glucose, fasting insulin, HbA1c - IGF-1 LR3 acts on the insulin receptor as well; hypoglycemia risk is real if dosed close to fasted training or long after a meal.
- IGF-1 (serum) - tricky here, because most assays don’t distinguish endogenous IGF-1 from LR3. Use it as a directional confirm rather than an exact dose-response.
- CBC, CMP - baseline kidney/liver as anywhere else.
Because IGF-1 LR3 is essentially a 4-week-blast tool with mandatory carb intake post- injection, the bracketing pattern is different from the GH axis - baseline, mid-cycle (week 2–3), and post-washout. The dose-strategy and risk framing for this compound class lives in the Lean Mass and Hypertrophy application; the on/off rationale lives in Cycling Strategies.
Healing peptides (BPC-157, TB-500/Thymosin Beta-4, GHK-Cu)
- CBC and CMP at baseline and ~12 weeks - mostly to catch unrelated issues that get blamed on the peptide. These compounds don’t typically move bloodwork at standard doses.
- VEGF (optional, niche) - BPC-157 is associated with VEGF upregulation. Most users skip this unless there’s a specific reason. Active malignancy is the contraindication, not a routine concern.
Melanocortin agonists (Melanotan II, PT-141)
- Resting blood pressure - the most relevant marker. PT-141 can produce transient BP increases; chronic MT-II use can shift baseline BP up. Track it weekly on protocol, not just before/after.
- CBC - standard.
- Skin survey (clinical, not a lab) - document existing nevi before any MT-II protocol. Photographic baseline beats memory.
Thymosin Alpha-1
- CBC with differential - the relevant signal is in the differential (lymphocytes, CD4 if you’re tracking immune tone). Most users only do a CBC; CD4 panels are clinic-level monitoring.
- hsCRP (optional) - inflammatory tone. Not a dose-response measure, but useful if you’re running Tα1 on top of an inflammatory baseline.
Cycle-pattern protocols and the broader immune-resilience framing live in the Immune Resilience application.
When to draw
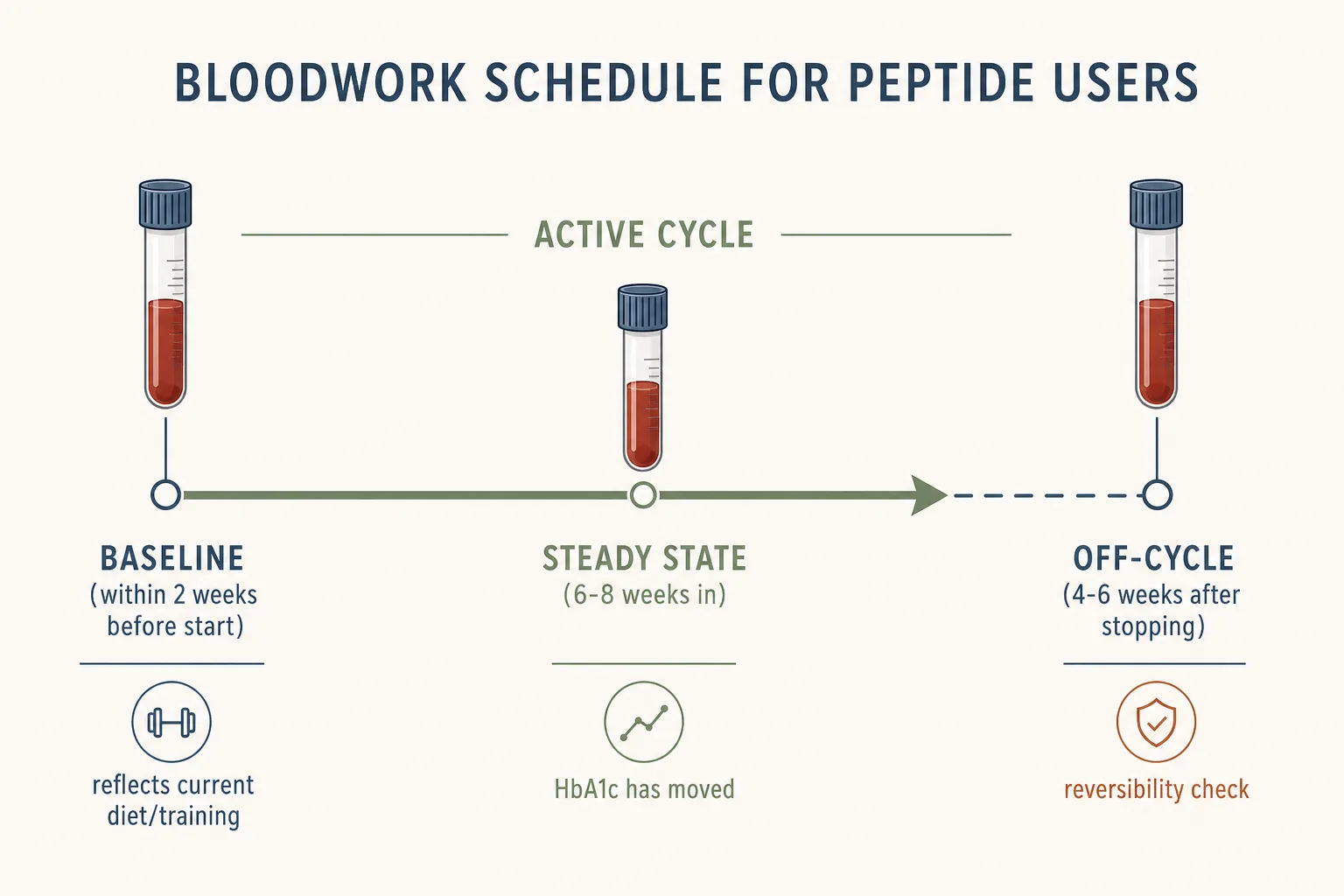
- Baseline: within two weeks before starting. Earlier than that and the number doesn’t reflect your current diet, training, and sleep state.
- Steady state: 6–8 weeks into a cycle. Long enough for HbA1c to move (it’s a 90-day rolling average), IGF-1 to settle, and weight-related changes to stabilize.
- Off-cycle: 4–6 weeks after stopping. Catches lingering effects and confirms reversibility for the markers that should reverse.
Always draw fasting (no calories for 12 hours) for glucose, lipids, and insulin. IGF-1 is not strictly fasting-dependent but a morning fasted draw simplifies the comparison across cycles.
What the numbers mean - quick reference
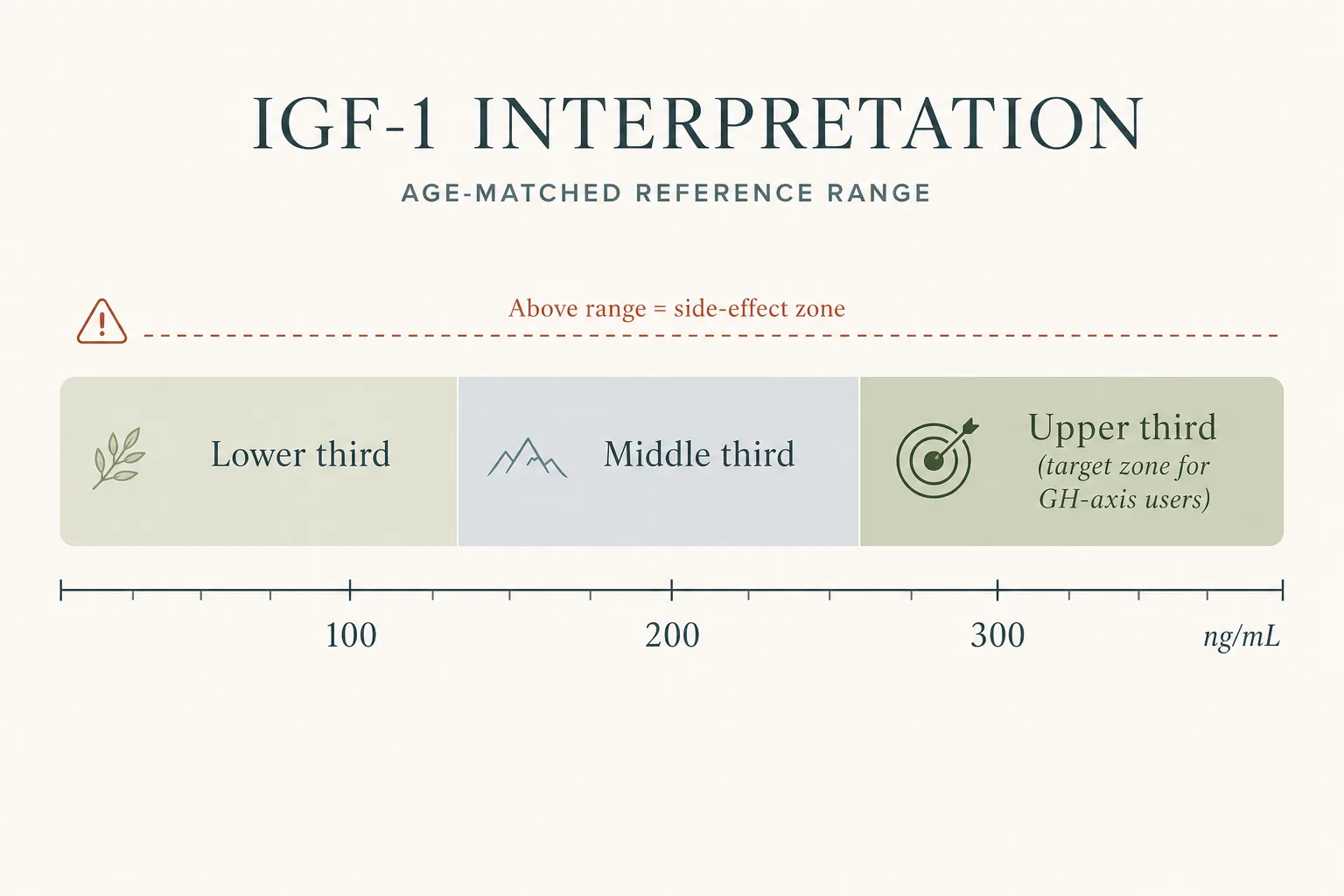
- IGF-1 in ng/mL. Adult reference range varies by lab, age, and sex. A common framing for GH-axis users: aim for the upper third of the age-matched reference range, not above it. “Above the range” is where the side-effect curve gets steep.
- HbA1c. Below 5.7% is the standard non-diabetic ceiling. Drift toward or above that on a GH-axis or somatropin protocol is the “back off” signal. On GLP-1 therapy expect HbA1c to fall.
- Fasting glucose. Below 100 mg/dL non-diabetic. 100–125 is pre-diabetic; sustained drift into that band on GH-axis use is meaningful.
- Hematocrit. Watch the upper end especially if you’re also on androgens. Above ~52% in men typically prompts a clinical conversation.
- LDL / triglycerides. Move with body composition; GLP-1 use usually improves both. Worsening on a GH-axis protocol is unexpected and worth investigating.
- Resting heart rate. A persistent 8–10+ bpm rise on retatrutide or any glucagon-active compound is a real signal. The discipline behind it - 14-day pre-protocol baseline, daily measurement, drift vs noise - is in Heart Rate as a Peptide Sentinel.
- Blood pressure. The sister sentinel to resting HR; moves in different directions for different classes (PT-141 transient pressor, GLP-1 modest dip, GH-axis edema-driven climb, MT-II bidirectional). Per-class numbers, home-cuff discipline, postural readings, and per-class stop thresholds are in Peptides and Blood Pressure.
How to actually order it
The friction-free path in the US is direct-to-consumer lab services (Marek, Quest direct, Labcorp’s OnDemand, Empower, Inside Tracker, Function, etc.) which let you bundle most of the markers above for $100–$300 depending on how much you include. In Europe, most countries allow direct-to-patient orders for the routine markers; the GH-axis labs (IGF-1) sometimes require a clinician request. A primary care physician will typically run a baseline CBC + CMP + lipids + HbA1c without questioning the indication; the hormone-axis labs are easier through a private endocrinology clinic or a peptide-friendly longevity practice.
Keep results in a single spreadsheet or PDF folder, organized by date and protocol. The comparison across cycles is where the real signal lives - not any single draw.
What this article doesn’t cover
Specialty endocrine workups (GH stim tests, OGTT for IGF-1 dynamics, full thyroid panels) are clinic-level investigations and out of scope here. Coagulation panels are not routinely needed for the peptides in this catalog. Genetic risk markers (APOE, MTHFR, etc.) are relevant to longevity discussions but don’t change how you run a cycle. The deeper insulin-sensitivity and HOMA-IR / CGM tooling that some of the per-class panels above point at - plus the fasting-window rule and how exogenous insulin reshapes peptide timing - is broken out in Peptides and Insulin.