There are three levers for pushing the growth hormone axis and five compounds that matter. They are not interchangeable. This playbook walks through what each one actually does, where it fits, what it costs in money and side effects, and how to pick between them.
The three levers
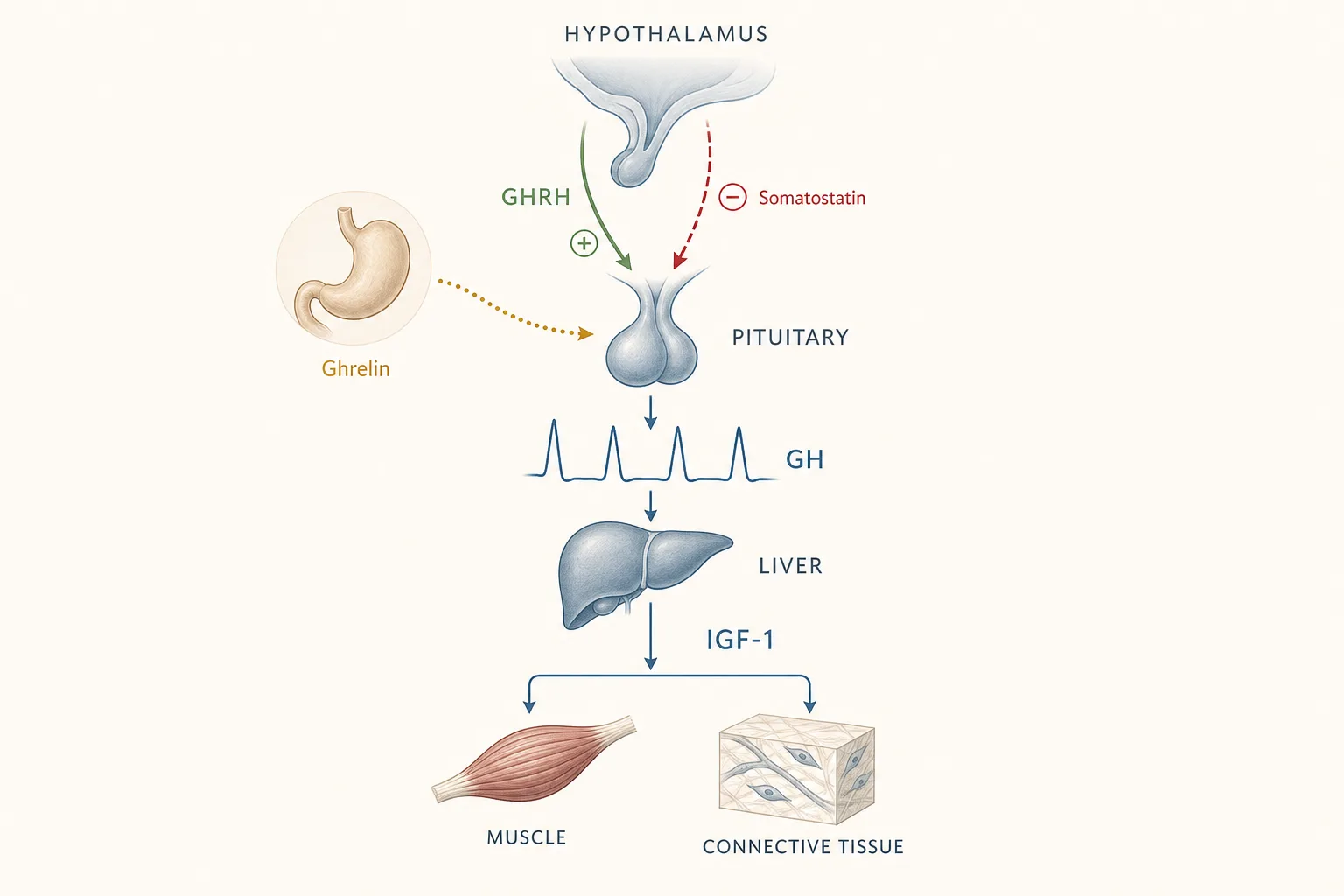
The pituitary releases growth hormone (GH) in pulses. Those pulses are gated by two hormones upstream - GHRH pushes the pituitary to fire; somatostatin tells it to stay quiet - and amplified by a third, ghrelin, which binds the GHS-R1a receptor. GH in turn drives IGF-1, mostly from the liver. Most of the anabolic, recovery and body-composition effects people chase are downstream of IGF-1, not GH itself.
You can intervene at three points:
- GHRH analogs - Mod GRF 1-29, CJC-1295 (DAC), Tesamorelin. Push the pituitary to release its own GH. Needs a working pituitary. Preserves feedback.
- GHRPs / GHS-R agonists - Ipamorelin is the relevant one here. Mimic ghrelin, amplify the pulse GHRH triggers, and blunt somatostatin. Useless alone in the way GHRH is - they work by potentiating a GHRH signal that’s already firing.
- Exogenous GH - Somatropin (rhGH). Skip the pituitary entirely. Delivers GH directly into circulation. Most powerful, most side effects, shuts down the native pulse.
The key reason to understand these three categories: GHRH and GHRP are synergistic. Running one of each produces a larger, cleaner GH pulse than doubling the dose of either. That’s why the default stack in practice is Mod GRF + Ipamorelin, not two of either.
The five compounds, head to head
Mod GRF 1-29
- Class: GHRH analog (first 29 amino acids of GHRH with four substitutions for injectable stability).
- Half-life: ~30 minutes. This is the point - it produces a single sharp pulse, then clears.
- Dose: 100 mcg per injection, typically 1–3x per day (fasted, usually pre-bed and/or post-workout).
- Pulsatility: High. Mimics a natural GHRH pulse.
- Cost: Cheap. A 5 mg vial covers weeks at 100 mcg/day.
- Side effects: Minimal at standard doses. Transient facial flush and mild injection-site reaction are the common ones.
- Who it’s for: Anyone who wants the GH axis nudged without committing to continuous elevation. The default GHRH choice when paired with Ipamorelin.
CJC-1295 (DAC)
- Class: GHRH analog with a Drug Affinity Complex that binds serum albumin.
- Half-life: 6–8 days. Once-weekly dosing is practical.
- Dose: 1–2 mg once per week.
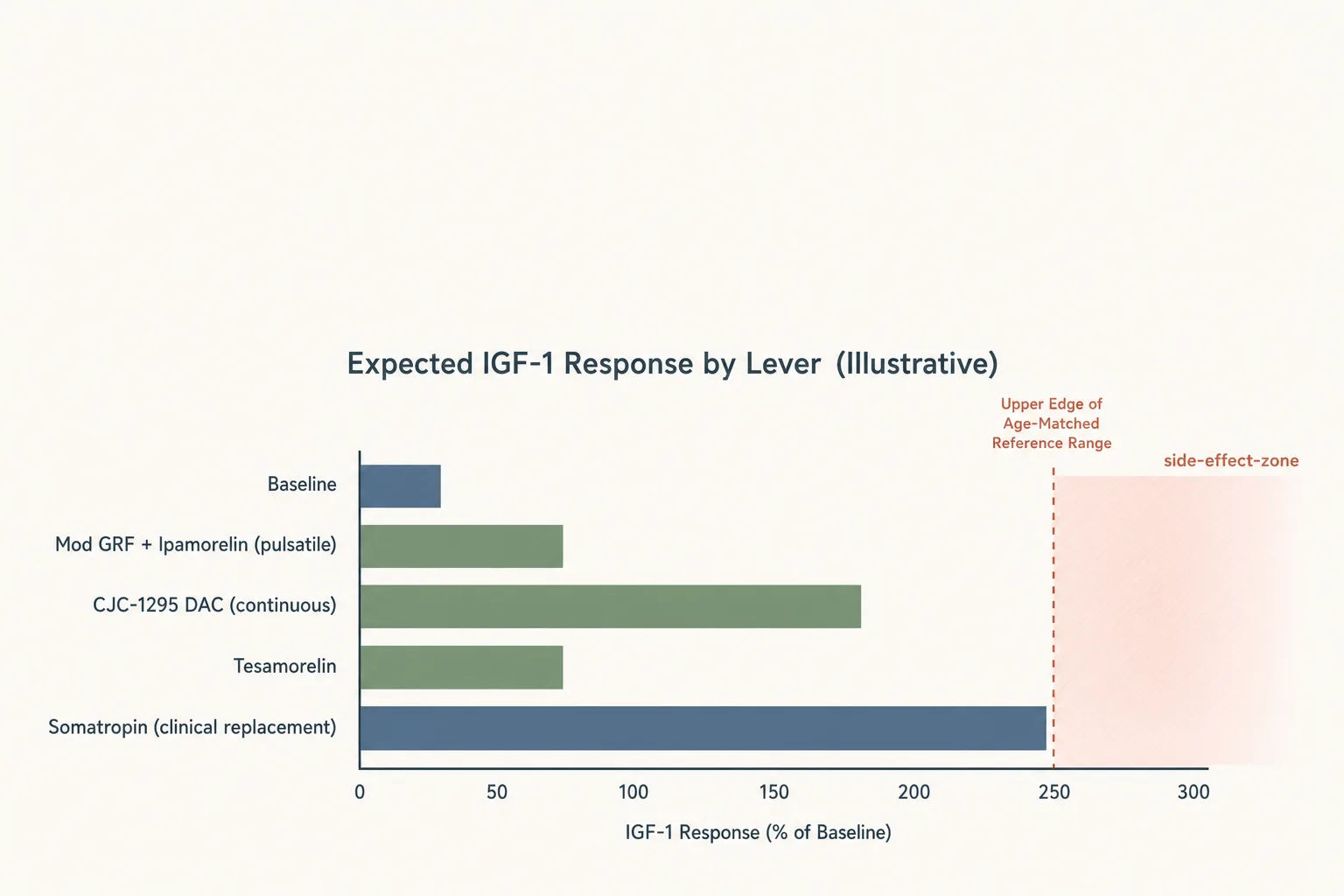
- Pulsatility: None - this is the important part. DAC creates a continuous “bleed” of GH release rather than discrete pulses. Total GH and IGF-1 area-under-curve go up, but the signal is flat, not rhythmic.
- Cost: Cheap per week.
- Side effects: More water retention, more tingling/numbness (CTS-pattern), and more potential for insulin-sensitivity drift than pulsatile GHRH. Because there’s no trough, the pituitary is under continuous stimulation.
- Who it’s for: Users who prioritise sustained IGF-1 elevation for hypertrophy or fat-loss goals over physiological pulse architecture, and who want the convenience of weekly dosing. Not the right tool if the goal is “feel like a better version of baseline.”
Ipamorelin
- Class: Selective GHS-R1a agonist (GHRP family). Ghrelin receptor agonist without the ghrelin-receptor appetite/cortisol/prolactin baggage seen with GHRP-2 and GHRP-6.
- Half-life: ~2 hours.
- Dose: 100–300 mcg per injection. 1–3x per day. Saturation is around 1 mcg/kg - past ~100 mcg you get longer duration, not a bigger peak.
- Pulsatility: High. Works by amplifying endogenous GHRH tone and inhibiting somatostatin, so the pulse shape stays natural.
- Cost: Cheap.
- Side effects: Cleanest in the GHRP class. Does not meaningfully raise cortisol or prolactin at standard doses. Mild hunger spike is possible but much less than GHRP-6.
- Who it’s for: Paired with a GHRH. Running Ipamorelin solo works - it will trigger the pulse - but you leave the synergy on the table.
Tesamorelin
- Class: GHRH analog. Full-length GHRH 1-44 with an N-terminal trans-3-hexenoyl group that extends in-vivo stability.
- Half-life: ~26–38 minutes subcutaneous.
- Dose: Clinical label is 2 mg/day (Egrifta, HIV-associated lipodystrophy). Community doses of 1 mg/day are common for general GH-axis work.
- Pulsatility: High - despite the bigger dose, clearance is fast and the pulse remains discrete.
- Cost: The most expensive item on this list by a wide margin. Order-of-magnitude more per cycle than Mod GRF.
- Side effects: Low. Best-characterised safety profile of any GHRH analog (it has the Phase III data the others don’t). Mild IGF-1 rise, occasional injection-site reaction, small HbA1c drift in some users.
- Who it’s for: Visceral fat specifically - this is the only peptide here with an FDA-approved indication for VAT reduction, and the trial data (~15–20% VAT reduction over 26 weeks) is the reason it exists. Also the right choice when you want a GHRH with actual human outcomes data and you can absorb the cost.
Somatropin (HGH)
- Class: Recombinant human growth hormone. Not a secretagogue - this is the hormone.
- Half-life: ~3–4 hours subcutaneous (absorption-limited).
- Dose: Clinical GHD replacement starts 0.1–0.3 mg/day titrated to IGF-1 and tolerance. Non-medical use is typically expressed in IU and runs significantly higher, with correspondingly higher risk.
- Pulsatility: None. Subcutaneous HGH produces a broad, flat GH elevation. The endogenous nocturnal pulse is suppressed by negative feedback during use.
- Cost: The most expensive option on a per-week basis once doses are meaningful, and the most counterfeited - IGF-1 bloodwork is effectively the only way to confirm potency.
- Side effects: The full list. Water retention, carpal tunnel symptoms, insulin resistance and fasting glucose rise, joint aches, and with chronic high-dose use the acromegaly-pattern tissue changes. These scale with dose and duration.
- Who it’s for: Diagnosed adult GHD under medical management is the clean case. In performance contexts, it’s the lever people reach for when secretagogues aren’t enough - usually alongside AAS and sometimes insulin, which compounds the risk stack. If your pituitary works, secretagogues will get you most of the effect most of the time at a fraction of the cost and risk.
Pulsatility, and why it keeps coming up
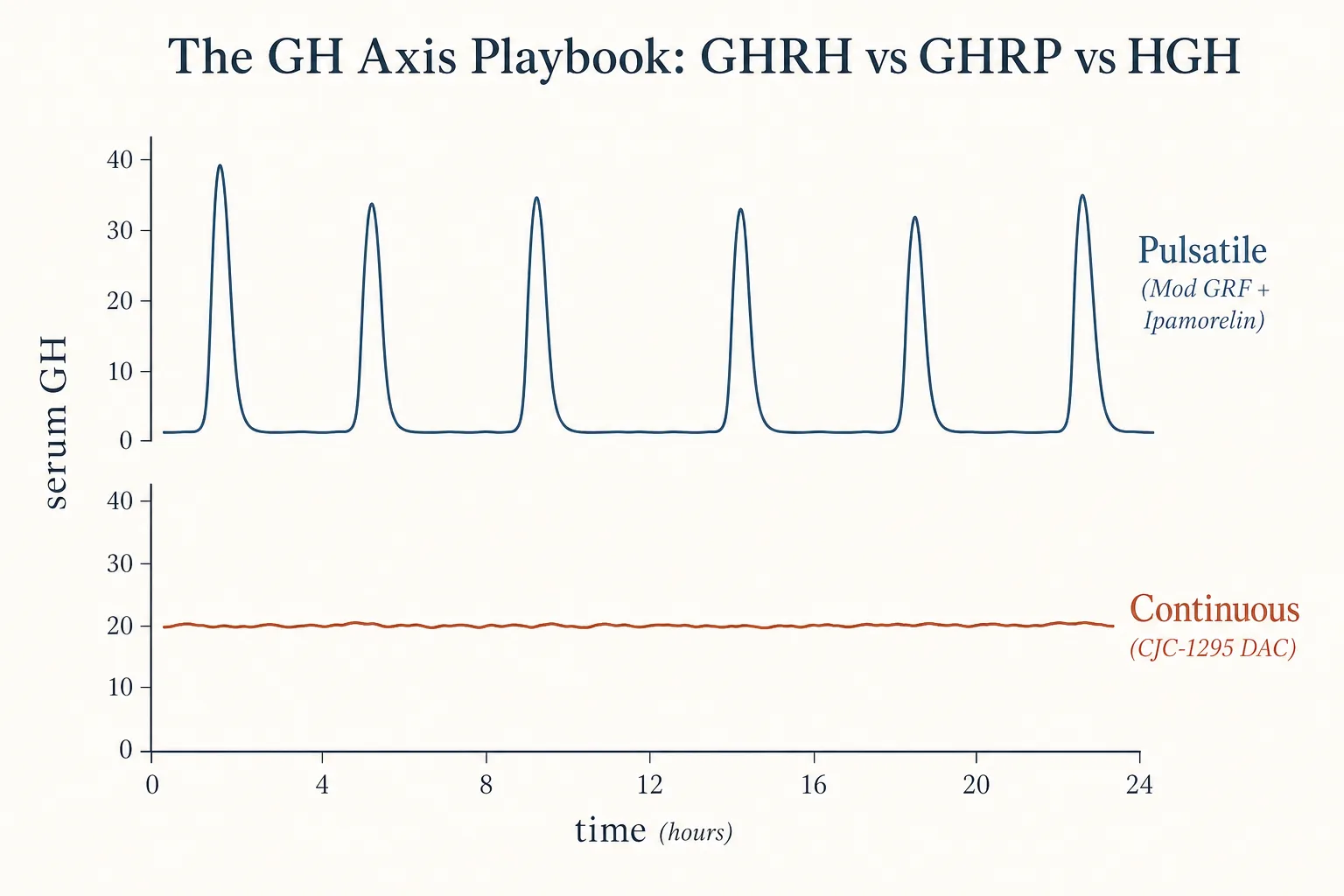
Endogenous GH is released in discrete pulses, mostly at night. Between pulses, GH is near zero. That pattern matters because receptors downregulate under continuous signal and because insulin sensitivity, lipolysis signaling, and IGF-1 feedback all evolved around the pulse-and-trough rhythm.
GHRH analogs with short half-lives (Mod GRF, Tesamorelin) and GHRPs (Ipamorelin) preserve that rhythm - they trigger a pulse and then get out of the way. CJC-1295 DAC and exogenous HGH don’t. That’s the structural reason side-effect profiles diverge as you move down the list: the further you get from “pulse and clear,” the more you lean on a system that doesn’t have a trough to recover in.
This is not an argument that continuous elevation is wrong - for a hypertrophy or VAT-reduction goal with a fixed cycle length, a higher AUC may be exactly what you want. It’s an argument that the choice is a real tradeoff, not a tier list.
The default stack
Mod GRF 1-29 100 mcg + Ipamorelin 100–200 mcg, taken together, once to three times per day on an empty stomach. This is the baseline protocol most practical GH-axis work is built around. The reasoning is clean: GHRH opens the gate, GHRP kicks the pulse harder, and both clear within an hour or two. Native pulses the rest of the day are undisturbed.
Timing matters. Insulin blunts GH release, so dosing is on an empty stomach - at least 2 hours post-meal, and no food for ~30 minutes after. Pre-bed is the highest-value slot because it stacks with the natural nocturnal pulse. The one-screen runbook for this stack (reconstitution, draw, fasting window, week-by-week expectations) lives in the Pre-Bed GH-Secretagogue Protocol guide.
Stacking Ipamorelin on top of Tesamorelin works the same way, just more expensive. Stacking Ipamorelin on top of CJC-1295 DAC is less clean - the DAC signal is already saturating the GHRH side, so you’re adding cost without the pulse architecture that makes the pairing interesting in the first place.
Cost reality
Rough per-month order of magnitude for a standard single-user protocol, grey-market sourcing:
- Mod GRF 1-29 + Ipamorelin daily: low two figures USD.
- CJC-1295 DAC weekly: low two figures USD.
- Tesamorelin 1–2 mg/day: mid-to-high three figures USD.
- Somatropin at bodybuilding doses: high three to low four figures USD, with significant counterfeit risk at the low end of that range.
Price alone doesn’t decide the choice, but the 20–50x gap between secretagogues and HGH is a real factor in how people ladder up.
Bloodwork minimum
Regardless of which lever: baseline and 6–8-week IGF-1, fasting glucose and HbA1c, and a full lipid panel. IGF-1 confirms the compound is doing something (and, in the HGH case, confirms it isn’t bunk). Fasting glucose and HbA1c catch the most common downside. Anyone running DAC or HGH for more than a cycle or two should also keep an eye on blood pressure and, if symptoms appear, consider carpal tunnel screening. The full per-class panel and timing rules live in Bloodwork for Peptide Users; the metabolic-side question - fasting-window timing, HOMA-IR, when CGM starts earning its keep - is broken out in Peptides and Insulin.
Decision tree
Start here and stop at the first “yes.”
- Is the goal specifically visceral fat reduction, and cost is not the
constraint?
→ Tesamorelin 1–2 mg/day, optionally with Ipamorelin 100 mcg. This is the only choice with direct human outcome data for VAT. Full goal-specific decision tree, stacks and monitoring plan in the dedicated Visceral Fat application. - Is the goal hypertrophy or aggressive recomposition, pituitary is intact, and
weekly-only dosing is a hard requirement?
→ CJC-1295 (DAC) 1–2 mg/week. Accept the side-effect and non-pulsatile tradeoffs. The Lean Mass and Hypertrophy application has the full evidence-tier sort across the GH axis, IGF-1 LR3 and the lower-evidence compounds, plus the AAS-context decision tree. - Is the goal general GH-axis optimization - sleep, recovery, body
composition, feel - with minimal side effects?
→ Mod GRF 1-29 100 mcg + Ipamorelin 100–200 mcg, pre-bed. Add a second daily dose post-workout if recomposition is the priority. - Is sleep specifically the goal?
→ Ipamorelin 100–200 mcg alone, pre-bed. A GHRP into an intact nocturnal GHRH signal is often enough, and avoids stacking cost for a single target. The full sleep-application decision tree (DSIP timing, Epitalon framing, sleep-hygiene prerequisites) lives in Sleep and Recovery. - Have you run a proper GHRH + GHRP stack for 8–12 weeks with sane
timing and bloodwork, and genuinely plateaued?
→ Only then does Somatropin become a rational next step. Start low (clinical-replacement range), titrate to IGF-1, and accept that the risk and cost profile is a category shift, not an increment.
What this playbook doesn’t cover
GHRP-2 and GHRP-6 are omitted deliberately - Ipamorelin covers the same mechanism cleaner. Hexarelin is omitted for receptor-downregulation reasons (the broader on/off framework for GH-axis compounds is in Cycling Strategies). MK-677 (Ibutamoren) is oral and non-peptide, so it sits outside scope here even though it pushes the same axis. IGF-1 LR3 bypasses the GH step entirely and belongs in its own writeup. Sermorelin is GHRH 1-29 unmodified - Mod GRF 1-29 supersedes it for most users.