Core formula
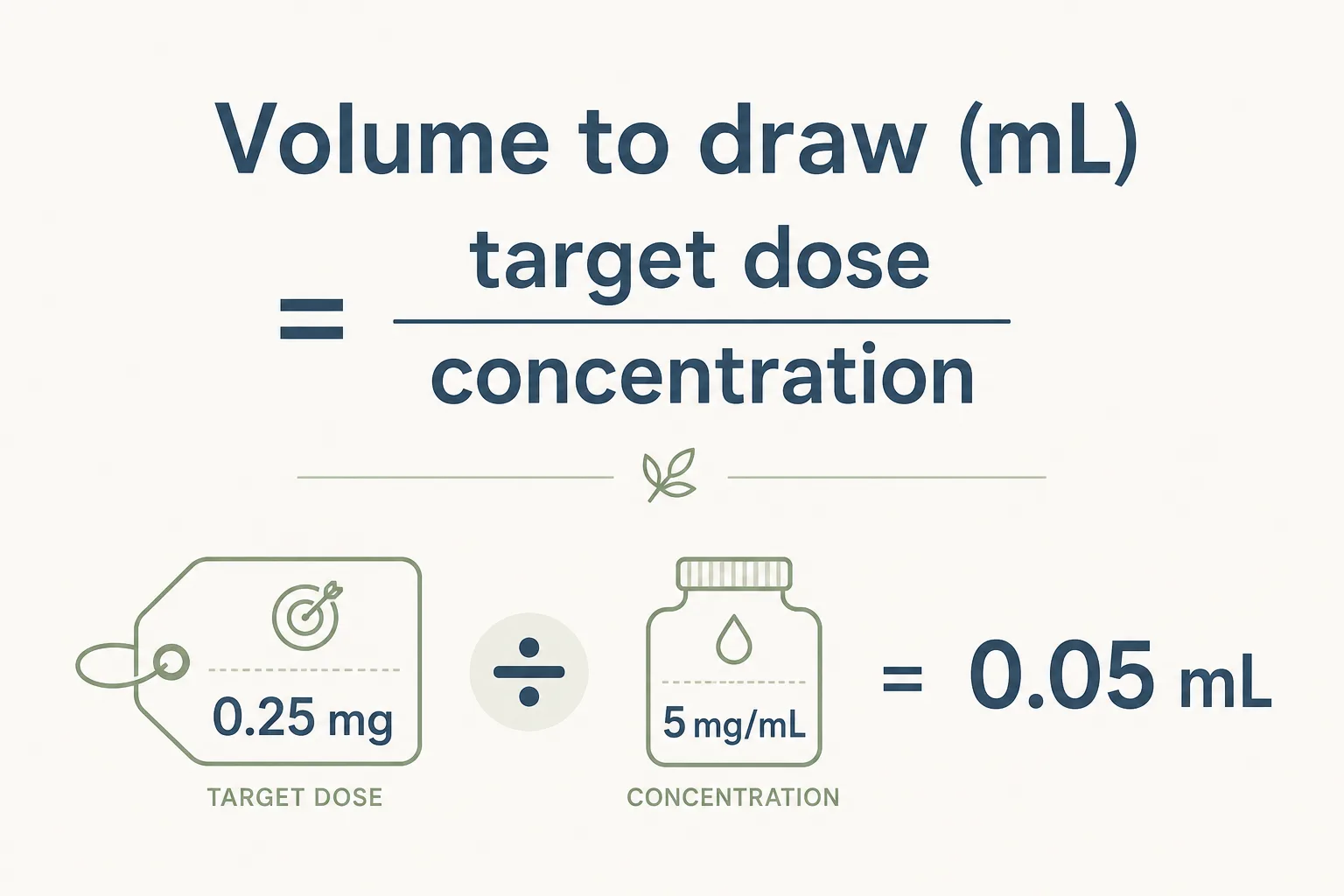
Volume to draw (mL) = target dose ÷ concentration.
If concentration is in mg/mL, target dose must be in mg. If concentration is in mcg/mL, target dose must be in mcg. Mixing units inside this formula is the most common 1000x error in the catalogue.
Unit conversions you must memorise
- 1 mg = 1000 mcg
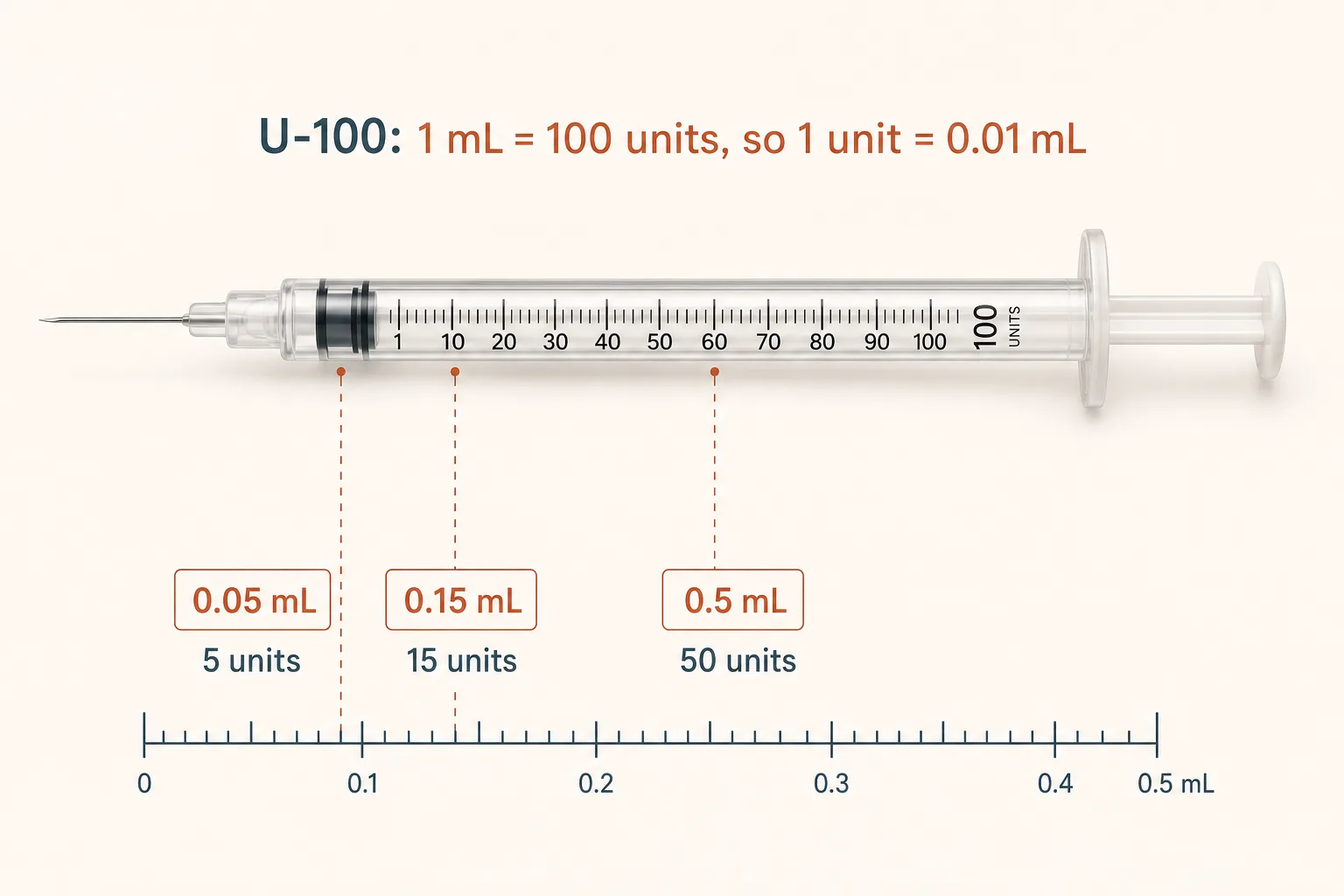
- U-100 insulin syringe: 100 units = 1.0 mL
- Therefore: 1 unit = 0.01 mL
For the lookup table (vial size × BAC volume → unit mark per dose), see Reconstitution Cheat Sheet. For the IU-vs-mg gotcha that comes up specifically with HGH, see Syringe Unit Conversions.
Picking the syringe
Most peptide doses are sub-1 mL. The default for SC peptide injection is the standard U-100 insulin syringe with an integrated short fine needle:
- 0.3 mL barrel for doses up to 30 units (most GH-axis, BPC-157, MT-II). Finest unit graduations on the smallest barrel; the most precise option for sub-30-unit draws.
- 0.5 mL barrel for doses up to 50 units (TB-500, larger BPC, IGF-1 LR3 reconstituted to 50 mcg/u).
- 1 mL barrel for full 100-unit draws (rare for SC peptides; more common for compounded GLP-1 vials drawn into a regular syringe).
- Needle: 29–31 G × 8 mm (5/16") is the default for SC. Smaller (31G) is more comfortable but kinks easier on tough skin. Avoid <28G for IM injections of larger volumes.
IM injections (rare in this catalogue - IGF-1 DES site enhancement, occasional TB-500) use a longer needle (1–1.5 inch / 25–38 mm) and a separate 1–3 mL syringe. The U-100 insulin syringe needle is too short for reliable IM in most adults.
Dead space - the silent dose loss
Every syringe has a small volume that stays in the hub between the plunger's bottoming-out and the needle tip - "dead space." For a 250 mcg dose drawn into a syringe with 0.05 mL of dead space at 50 mcg/u concentration, you lose ~10 mcg per injection (4% of dose) into the syringe waste.
- Integrated-needle insulin syringes have minimal dead space (~0.02–0.05 mL). The default choice for peptide dosing for this reason.
- Detachable-needle syringes (Luer-lock) can have 0.07–0.1 mL of dead space. Acceptable for high-volume IM injections where the dose-loss percentage is small; problematic for sub-50-unit SC peptide doses.
- Higher concentration helps. Drawing 100 mcg from a 50 mcg/u solution (2 units) loses more proportionally to dead space than from a 10 mcg/u solution (10 units). Reconstitution-volume decisions and dead-space considerations are linked.
Worked example 1 (mg-based)
Given concentration = 5 mg/mL, target dose = 0.25 mg:
- mL to draw = 0.25 ÷ 5 = 0.05 mL
- On a U-100 syringe: 0.05 mL = 5 units
Worked example 2 (mcg-based)
Given concentration = 2000 mcg/mL, target dose = 300 mcg:
- mL to draw = 300 ÷ 2000 = 0.15 mL
- On a U-100 syringe: 0.15 mL = 15 units
Worked example 3 (from vial amount)
Vial contains 10 mg total, reconstituted with 2 mL total volume.
- Concentration = 10 ÷ 2 = 5 mg/mL
- Target 1 mg dose → 1 ÷ 5 = 0.2 mL → 20 units on U-100
Worked example 4 (HGH IU)
Vial contains 10 IU somatropin, reconstituted with 1 mL BAC water.
- Concentration = 10 IU/mL = 0.1 IU per insulin-syringe unit
- Target 2 IU dose → 2 ÷ 0.1 = 20 units on U-100
- (In mg terms: 10 IU = ~3.33 mg, so concentration = ~3.33 mg/mL, target = 0.667 mg → 0.667 ÷ 3.33 = 0.2 mL = 20 units. Same answer by either path.)
Drawing technique
- Wipe the septum with 70% IPA and let it air-dry. Same protocol as reconstitution. See Storage and Handling Best Practices.
- Pull a small amount of air into the syringe first. Equal to or slightly more than the volume you'll draw. Inject the air into the vial headspace before pulling the dose - this prevents the vacuum that makes large draws stutter and air-bubble.
- Invert the vial. Needle tip goes into the liquid pool, not the headspace.
- Pull slowly, past your target volume. A few units over, then push back to the exact target unit mark. The push-back pass is what removes air bubbles that follow a fast pull.
- Tap to clear bubbles. Gently - flick with a fingernail. Push the air back into the vial, re-pull as needed.
- Read the unit mark at eye level. Plunger leading edge against the mark, not trailing edge of the rubber stopper.
- Cap the needle. Don't recap the same needle by pinching it back into the cap - you'll stick yourself. Set the cap on a flat surface and slide the needle in horizontally.
Backfill technique (high-volume / multi-vial draws)
For draws over 0.5 mL, or when drawing two compounds into one syringe (Mod GRF + Ipamorelin pre-bed, common stack):
- Draw the first compound to its target volume normally.
- For the second compound: don't pre-load air into the syringe. Insert the needle into the second vial, invert, pull the additional volume you need. The first compound stays in the syringe; the second adds on top.
- Watch for air at the meniscus between the two compounds. A few seconds of vertical stand lets it rise; tap to clear before injection.
Error-prevention checklist
- Write every step, including units, before drawing.
- Never mix mg and mcg in the same step without explicit conversion.
- Double-check concentration after any change in reconstitution volume.
- Re-read the unit mark after the draw and before injection - the second look catches the slip.
- Track dose number per vial in a log. The 14th dose feels routine; the routine is when the math gets sloppy.
Common pitfalls
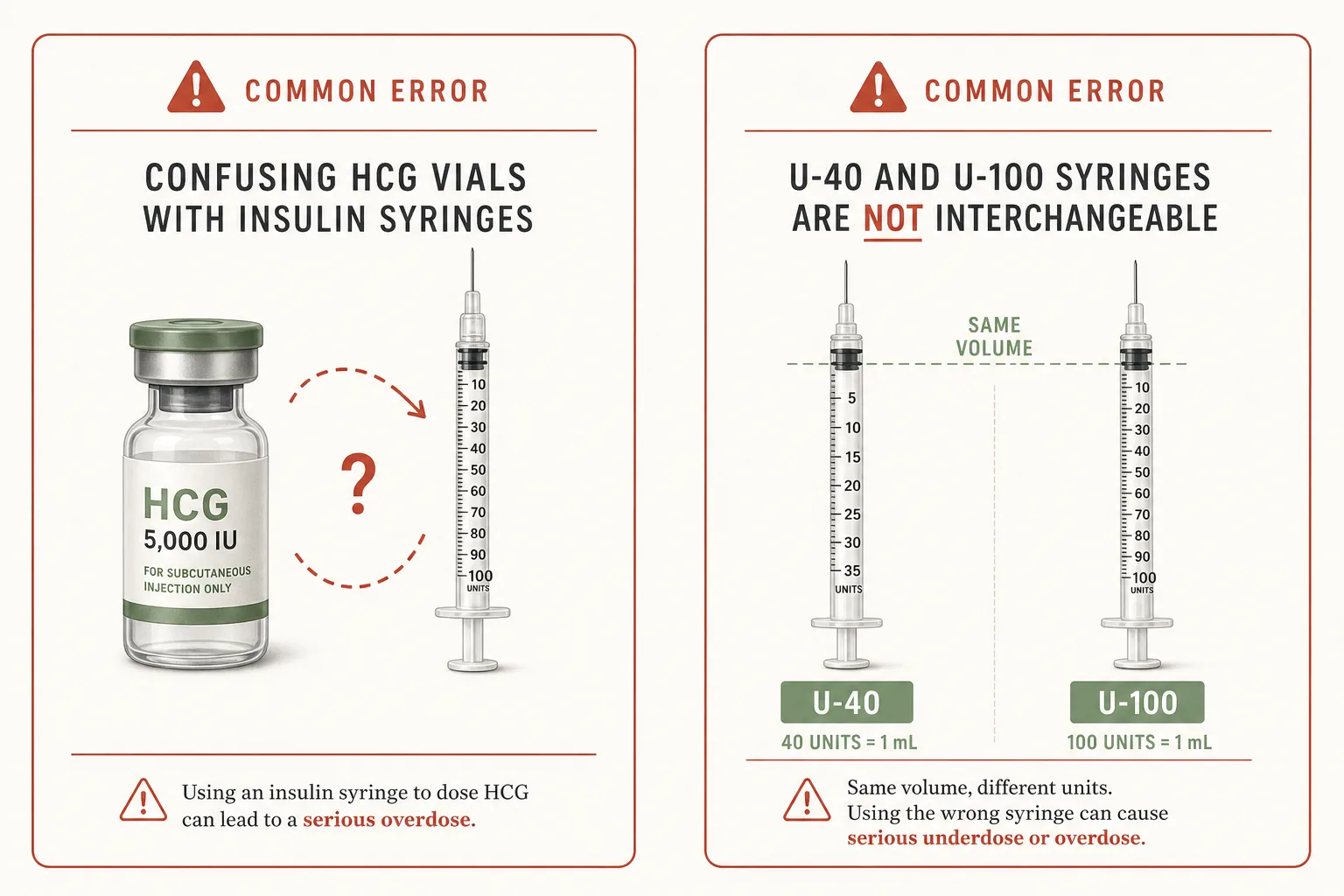
- Confusing syringe "units" with drug "units". An insulin-syringe unit is 0.01 mL. A "drug unit" (HGH IU, HCG IU, insulin IU) is a potency measure that depends on the drug. They are not interchangeable. See Syringe Unit Conversions.
- Using U-100 assumptions on a non-U-100 device. U-40 and U-100 syringes look similar but have different unit-to-mL ratios (40 vs 100 units per mL). U-100 is the default; if a U-40 appears, verify before drawing.
- Rounding too aggressively for small volumes. A 12.5 unit dose on a U-100 (which only graduates whole units) is a real decision: round to 12 or 13 units, or change reconstitution volume so the dose lands on a whole unit. Don't pretend the syringe reads half-units when it doesn't.
- Drawing from the wrong vial. Mod GRF and Ipamorelin fiolas look identical once relabelled. Side-of-vial labelling discipline (date + concentration + compound name) prevents this. The common pre-bed-stack failure pattern.
- Skipping the second look. One quick re-read of the unit mark before the injection catches the slip. Five seconds; high return.
Sources
- ISMP: Preventing medication errors with injectable products - https://www.ismp.org/recommendations
- FDA resources on insulin products and concentration labeling - https://www.fda.gov/drugs/drug-safety-and-availability/information-about-insulin-products
- CDC Injection Safety basics - https://www.cdc.gov/injection-safety/about/index.html