Scheduled surgery - orthopedic repair, sports-injury reconstruction, abdominal procedure, dental implant - is one of the cleanest operator scenarios for a peptide protocol. The injury is dated, controlled, and observed; the recovery has a known timeline; the operator has a 2-4 week pre-op window to set baseline. This article walks through the pre-op set-up, the wash-out and disclosure questions, the post-op compound stack worth considering, and the failure modes that come from running healing peptides too aggressively in a context that has its own clinical guardrails.
The framing
This article is for users planning peptides around their own surgery. The decisions are operator-grade but the context is medical: there's a surgical team, an anesthesia provider, and a recovery protocol that the peptide stack sits on top of - not beside. The right way to engage with that team is straightforward disclosure, not concealment. Surgeons who practice in any sports- medicine or aesthetic-medicine adjacent space see BPC-157 / TB-500 often enough that the conversation isn't unusual.
Pre-op: the 2-4 week set-up window
The pre-op window is the cleanest opportunity to lay baseline and decide which compounds will run post-op. Don't start a new peptide for the first time inside this window - first cycles need a longer read than 2-4 weeks gives, and surgery itself is the variable you want to study.
- Bloodwork baseline. CBC, CMP, lipids, HbA1c, IGF-1 minimum. Useful as the reference for post-op recovery monitoring; many of these will be re-pulled by the surgical team anyway. See Bloodwork for Peptide Users.
- Body-comp + photographic baseline. Useful both for tracking recovery progress and for any cosmetic-recovery application. Day-zero photos of the surgical area are worth pulling before the team takes their own.
- Resting heart rate + BP for 14 days. Anesthesia and surgery shift autonomic tone; a clean 14-day pre-op baseline makes the post-op trend interpretable. See Heart Rate as a Peptide Sentinel.
- Don't start peptides for the first time. Run the trial-and-error cycle elsewhere. The pre-op window is for confirming that compounds you've already validated work for you.
Wash-out timing for compounds running into surgery
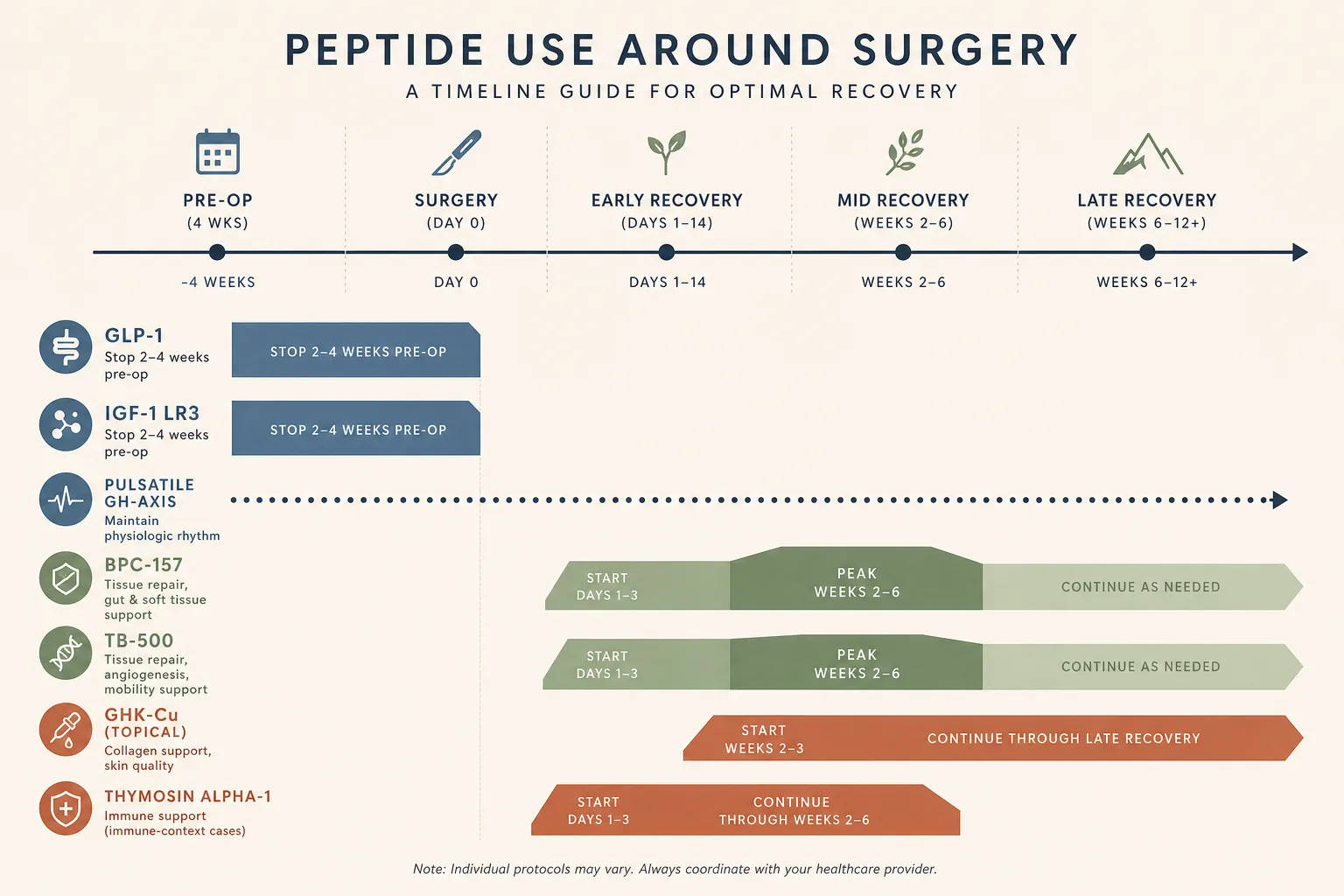
- GLP-1s and tirzepatide: the one with active surgical guidance. The American Society of Anesthesiologists has published guidance recommending withholding daily GLP-1s the day of surgery and weekly GLP-1s for at least one week pre-op, because of delayed gastric emptying and aspiration risk under anesthesia. Surgical centers vary in how strictly they follow this; the disclosure-first answer is to ask the anesthesia provider what they want.
- BPC-157 and TB-500. No specific surgical guidance exists. Most operators discontinue 1-2 weeks pre-op out of caution about angiogenesis interfering with surgical-site coagulation; some teams are comfortable with continued use right through. The asymmetry: stopping is reversible, continuing isn't, so the conservative path is the default unless the team has explicitly approved continuation.
- GH-axis compounds (Mod GRF + Ipamorelin, Tesamorelin, Somatropin). Continuous-elevation GH (DAC, exogenous HGH) shifts insulin sensitivity and fluid balance enough to matter under anesthesia; pulsatile stacks less so. Wash out continuous-elevation compounds 2-4 weeks pre-op; pulsatile stacks can often run through with disclosure.
- IGF-1 LR3. Hypertrophy-tier compound; not something to be running into surgery. Stop at least 4 weeks pre-op.
- Melanocortin agonists (PT-141, MT-II). Transient pressor effects don't combine well with anesthesia. Discontinue at least 1 week pre-op.
Disclosure: what to tell the surgical team
- Be specific by compound name. "I take some peptides" is not useful. "I run BPC-157 250 mcg SC twice daily, last dose two weeks before surgery" is. The team can't reason about generalities.
- The pre-op questionnaire is the right vehicle. Most modern surgical centers ask about supplements, herbals, and research compounds. Use that field. If the form doesn't have a field for it, write it in.
- The anesthesia provider is the relevant audience. They make the day-of decisions about NPO status, drug interactions, and intra-op monitoring. The surgeon cares about the surgical-site question (BPC, TB-500); the anesthesia provider cares about the systemic question (GLP-1 gastric emptying, GH-axis fluid balance).
- If continuing through surgery is on the table, get explicit sign-off. "I'd like to continue BPC-157 because of the post-op recovery thesis - is there any reason from your side I shouldn't?" The conversation is short; the cost of skipping it is real if something goes sideways.
The post-op stack worth considering
Post-op repair is the strongest evidence-tier scenario for the healing peptides in this catalog. The proliferation phase (days 3-14 post-op) is exactly the rate-limited window the BPC + TB synergy targets.
- BPC-157 + TB-500 (the default healing pair). BPC-157 250-500 mcg SC twice daily, ideally near the surgical site for orthopedic procedures, beginning when wound closure is sealed enough to inject. TB-500 4-5 mg per week loading for 4-6 weeks, then 2-2.5 mg per week maintenance until functional return. See BPC + TB synergy.
- GHK-Cu for scar minimization. Topical 1-2% cream on the closed incision once a day starting at 2-3 weeks post-op (after sutures or staples are out and the incision is sealed). Works on the remodeling phase rather than the early repair phase. Systemic GHK-Cu adds to the picture but topical captures most of the cosmetic-recovery benefit.
- Thymosin alpha-1 if immune-context is real. Major surgery suppresses immune tone for 1-3 weeks post-op. Tα1 1.6 mg twice weekly during that window is reasonable for users with a real immune-recovery concern (older patients, those with prior infection complications, those facing a large procedure). Not necessary for healthy users undergoing routine procedures.
- GH-axis stack for slow healers or older patients. Mod GRF + Ipamorelin pre-bed during the 6-12 week recovery window adds a measurable IGF-1 contribution to collagen synthesis. The marginal benefit is largest in users over 50 or those with otherwise compromised recovery; younger users with intact GH tone get less out of it. See GH Axis Playbook.
- Oral BPC-157 for abdominal-surgery-context gut inflammation. Post-op ileus and the gut inflammation that follows GI surgery are both areas where oral BPC has documented activity. 250-500 mcg orally twice daily for 2-4 weeks post-op, paired with the standard surgical-team nutrition plan. See Gut Health.
Failure modes specific to surgery context
- Starting BPC + TB before the wound is sealed. Angiogenic compounds in an open wound increase bleeding risk and can interfere with primary intention healing. Wait for the surgical team's "wound is closed" signal - usually 7-10 days for ortho, longer for abdominal.
- Aggressive dosing as if the surgery were a worse injury than it is. Surgical procedures produce controlled, dated tissue insults. The dose ranges that fit a chronic-tendinopathy or multi-site soft-tissue protocol are too high for clean post-op healing. Stay in the standard ranges, not the upper end.
- Returning to load too fast because the peptide stack "worked." Subjective recovery is faster than tissue recovery. The peptides accelerate the underlying repair, but the surgical team's milestone-based return-to-load schedule still runs the calendar. Trying to compress that schedule because you feel good is the most common way users earn a re-injury.
- Cancer-history blind spot. Same as the standard BPC + TB caveat, but with extra weight: surgery often happens in contexts (resection, biopsy, mass removal) where the cancer question is the whole reason for surgery. Angiogenic compounds are explicitly contraindicated in those contexts. See Cancer Risk and Growth Factors.
- NPO violation. Most surgeries require 8-12 hours of nothing by mouth pre-op. SC peptides aren't "by mouth" in the literal sense, but the day-of-surgery answer is to follow whatever the anesthesia provider's instructions say.
Common cautions
- Surgical-site infection trumps the protocol. Any sign of post-op infection (fever, drainage, increasing redness past day 4, opened wound) is a stop signal for the peptide stack until the team has cleared the infection. Adding angiogenic / migration compounds during active infection can spread the wrong cells to the wrong place.
- Anticoagulation interaction. Many surgeries come with post-op anticoagulant prescriptions (heparin / DOACs). BPC-157 and TB-500 have no documented direct interaction with anticoagulants, but the surgical team is the right channel for "is this combination OK" rather than community forums.
- Insurance and billing context. Disclosing research-chemical use on a surgical questionnaire is the right move; it's also worth knowing that prescription channels (compounding pharmacies, GLP-1 prescriptions) leave a paper trail insurance can read. Most won't care about peptides; some occupational coverage might. Worth checking in advance for users in regulated professions.
What this article doesn't cover
Specific surgical procedures and their idiosyncratic recovery protocols (cardiac, neurosurgical, oncological resection) are out of scope - the operator answer there is "follow the surgical team's lead, peptides are not the load-bearing variable." Cosmetic / aesthetic procedures (filler, neuromodulators, skin resurfacing) follow a different timeline and a different stack emphasis (more GHK-Cu topical, less systemic) that warrants its own piece. Trauma surgery and unscheduled procedures don't have the pre-op window this article assumes; the post-op portion still applies but the planning side is different. Pediatric surgery is not in scope - the audience here is adult.
Cross-references
- Injury Recovery - the broader application this article specialises into the surgical context.
- BPC + TB synergy - the mechanism story behind the post-op default pair.
- Skin and Hair - GHK-Cu topical detail relevant to the scar-minimization application above.
- GH Axis Playbook - when adding a pulsatile GH stack to post-op recovery makes sense.
- Bloodwork for Peptide Users - the panels for pre-op baseline and post-op monitoring.
- Cancer Risk and Growth Factors - the contraindication context for surgeries that are themselves cancer-related.
- Gut Health - oral BPC-157 in the abdominal-surgery recovery context.