“Wolverine stack” gets named in every injury-recovery conversation, and most coverage stops at “they work better together.” The actual synergy thesis is more interesting and more qualified: the two compounds rate-limit different steps of the same repair process. Stacking them isn’t additive in a generic sense - it’s sequential in mechanism, parallel in time. This article walks through why, where the synergy is real, and where the story gets oversold.
For the application-level "what stack do I run for my torn rotator cuff" framing, see Injury Recovery. For the broader risk frame on angiogenic / migration peptides, see Cancer Risk and Growth Factors.
What each one rate-limits
BPC-157 - angiogenesis and fibroblast activation
- Upregulates VEGF (vascular endothelial growth factor) expression in injured tissue, driving new capillary formation. New blood supply is what gets nutrients and oxygen to the repair site.
- Activates fibroblasts - the cells that lay down collagen. Without sufficient fibroblast activity, even a perfectly vascularised injury heals slowly.
- Modulates nitric oxide signalling, which contributes both to vasodilation (more blood flow) and to growth-factor signalling cascades.
- Acts locally in the inflamed tissue when injected systemically - the angiogenic and fibroblast effects concentrate where the inflammation signal is strongest.
TB-500 (thymosin β-4 fragment) - cell migration and actin remodelling
- Sequesters G-actin monomers, regulating the dynamic balance between G-actin (free) and F-actin (filamentous). This is the cytoskeletal infrastructure cells use to physically move through tissue.
- Promotes cell migration - satellite cells, fibroblasts, and immune cells physically travel to the repair site. The migration step is genuinely rate-limiting for tendon and ligament repair, where local cell density is low at baseline.
- Modulates inflammation by regulating immune-cell trafficking; the "TB-flu" malaise some users report is consistent with this immune- modulation profile.
- Acts more systemically than BPC-157 - the cell-migration signal isn’t as gated by local injury markers.
Why stacking is more than additive
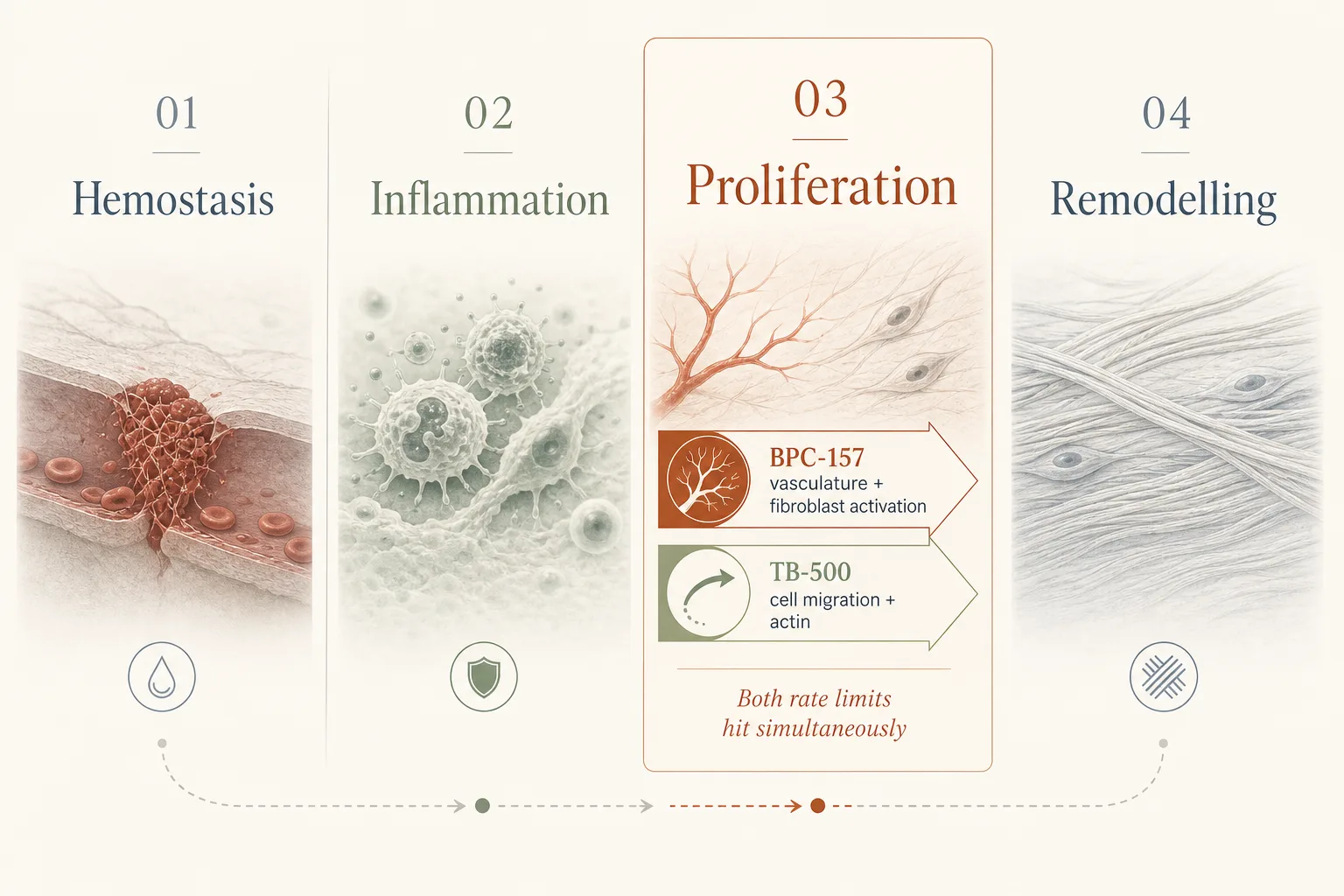
Tissue repair has roughly four phases: hemostasis, inflammation, proliferation (the cell-migration + collagen-laying phase), and remodelling. The proliferation phase has two parallel rate limits that the BPC + TB pair happens to address simultaneously:
- Cells need to arrive. TB-500 accelerates the migration step.
- Cells need infrastructure to work in. BPC-157 ensures the vasculature and fibroblast activation are in place when those cells arrive.
Running TB-500 alone speeds up cell arrival but the cells reach a poorly-vascularised, fibroblast-quiet site - the bottleneck shifts downstream. Running BPC-157 alone builds the infrastructure but waits longer for cells to populate it. Running both addresses both rate limits in parallel; this is the mechanistic basis for the synergy claim.
Where the synergy thesis breaks down
- Outside tendon / ligament / muscle context. The cell-migration bottleneck matters most where local cell density is low at baseline (avascular or hypovascular tissues). For wounds with plenty of local cell traffic anyway, the TB-500 contribution flattens.
- Acute vs chronic injury. The synergy framing comes from acute-injury repair. Chronic tendinopathy is partly a failed-remodelling problem, not a proliferation bottleneck. BPC + TB in chronic tendinopathy is a reasonable bet but doesn’t recreate the same mechanism.
- Animal-data dose translation. Most BPC + TB synergy data is rat / equine. Human dose-response curves aren’t cleanly mapped from those species, especially for BPC-157 where the gastric-juice-stable property doesn’t fully translate to systemic SC pharmacokinetics in humans.
- The pair both have angiogenic activity. TB-500 is also angiogenic via different mechanism (Tβ4 promotes endothelial cell migration and tube formation). The angiogenic load of the pair is greater than either alone - relevant for the cumulative-exposure cancer-risk frame.
Practical protocol implications
- Loading phase BPC + TB matters more than maintenance. The proliferation phase is days 3–14 post-injury for acute tissue trauma. Front-loading both compounds in that window captures most of the synergy benefit. Maintenance dosing past week 4 is optional.
- Local BPC + systemic TB. Some operators inject BPC-157 close to the injury site for theoretical local concentration advantage, while running TB-500 systemically because its mechanism works systemically. Mechanistically defensible; the local-BPC benefit over systemic-BPC is debated.
- Cycling the pair. Standard 4–8 weeks on, equal washout. Both are angiogenic; the cumulative exposure framework in Cycling Strategies applies to the pair, not just to BPC alone.
- Don’t stack BPC + TB year-round. The standard mistake. Both are tools for an injury window or a procedure- recovery window, not background “youth maintenance.” See Anti-Aging Stack for the broader frame on what does and doesn’t belong in a routine protocol.
Stack timing for typical use cases
| Use case | BPC-157 | TB-500 | Duration |
|---|---|---|---|
| Acute tendon strain | 250–500 mcg BID SC, optionally local | 2.5 mg twice weekly SC (loading), then 2 mg weekly | 4–6 weeks loading, then taper |
| Post-surgical recovery | 500 mcg BID SC for 2 weeks, then 250 mcg BID | 2.5 mg twice weekly for 4 weeks, then 2 mg weekly | 4–8 weeks bracketing surgery |
| Chronic tendinopathy | 250 mcg BID SC, optionally local | 2 mg weekly SC | 6–8 weeks; reassess |
| Maintenance / "training resilience" | Not indicated | Not indicated | Don’t run continuous |
What stops people
- Running the stack year-round as a wellness baseline. The proliferation-phase synergy is a tool for an injury or procedure window. Continuous use compounds the angiogenic-exposure risk without producing proportional benefit.
- Skipping the loading phase. Most of the mechanistic benefit lives in the days 3–14 proliferation window. A trickle-dose protocol misses the timing.
- Cancer history blind spot. The pair is contraindicated for active or recent cancer. Both compounds accelerate processes (angiogenesis, migration) that solid tumours also depend on. See Cancer Risk and Growth Factors.
- Assuming "more is more" past 2.5 mg TB-500 twice weekly. The dose-response curve flattens; doubling the dose doesn’t double the effect, just doubles the systemic load and cost.
- Counterfeit TB-500 specifically. The full-length Tβ4 is hard to manufacture stably; many grey-market "TB-500" products are short fragments with limited or no activity. Failure to respond is sometimes a sourcing problem, not a protocol problem. See Sourcing and Verification.
Cross-references
- Injury Recovery - the application-level decision tree for stacking BPC, TB, and adjunct compounds.
- Cycling Strategies - the on/off rationale for both compounds.
- Cancer Risk and Growth Factors - the per-mechanism risk frame for the angiogenic / migration pair.
- Skin and Hair - TB-500 in post-procedure recovery contexts (microneedling, laser, surgery).
- Peptides Around Surgery - the surgical-context specialisation: pre-op set-up window, anesthesia washout per compound, the post-op timing detail the table above abstracts over.
- Peptides for Endurance Athletes - where BPC + TB use is structured around volume blocks and connective-tissue overload patterns rather than discrete acute injuries.