BPC-157, TB-500, IGF-1 LR3 and GHK-Cu are some of the most-used compounds in this catalogue, and they share a question that users tend to hand-wave too quickly: do they cause cancer, or accelerate cancer that’s already there? The honest answer is three different things at once, because the underlying biology is three different mechanisms collapsed into one anxious word.
This article splits the “cancer concern” into the mechanisms it actually maps to, gives the evidence we have for each, and lays out a pre-cycle screen that takes one bloodwork session and turns the rest of the protocol into a much more defensible decision.
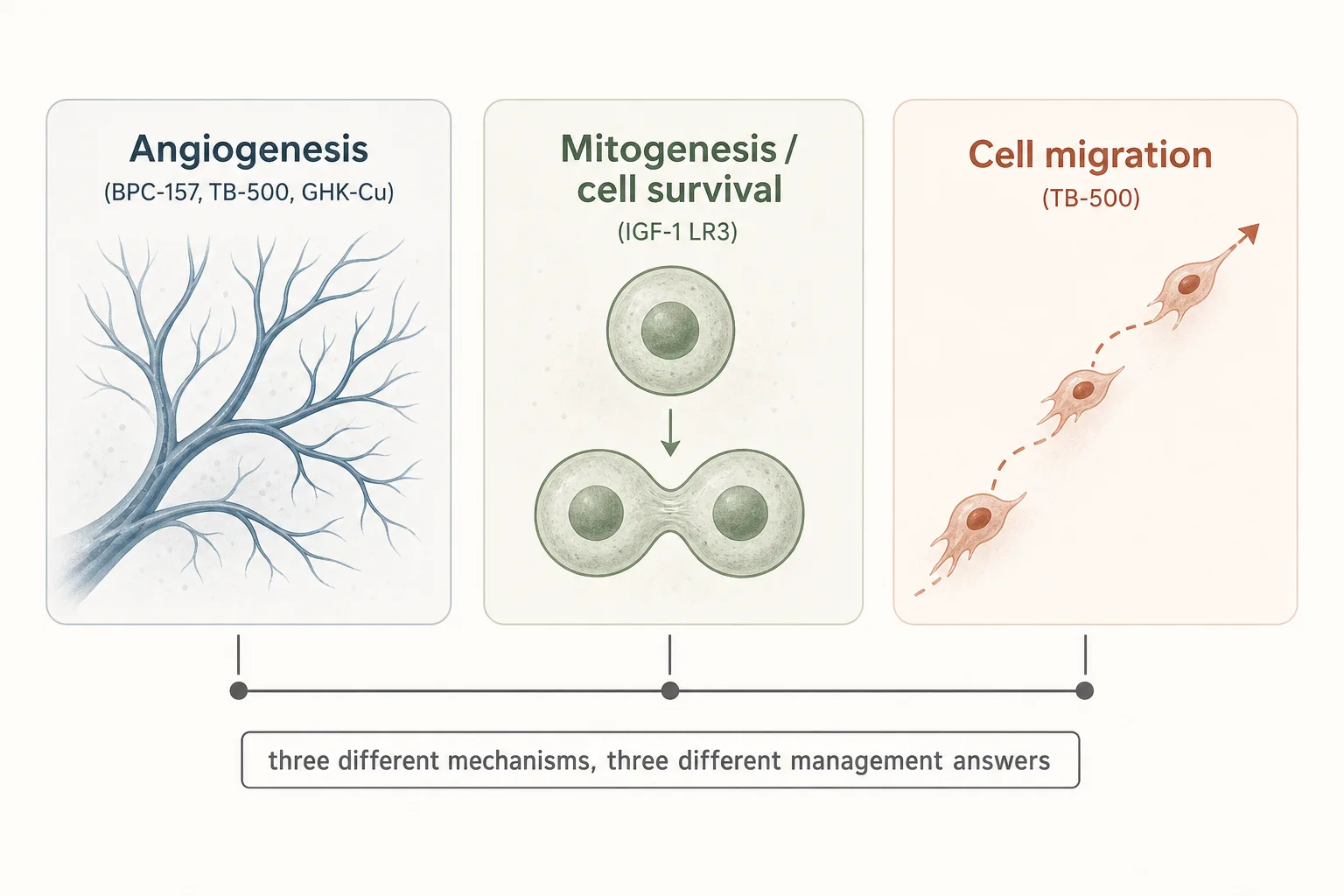
The three mechanisms, separately
When someone says “peptide X is a cancer risk”, they could mean any of the following. The risk-management answer is different for each.
1. Angiogenesis promotion
- What it is. Stimulating the growth of new blood vessels. BPC-157 upregulates VEGF as part of its tendon- repair mechanism. GHK-Cu is also pro-angiogenic in skin and wound healing, with the wrinkle that it has documented DNA-repair activity that partially counter-balances the concern.
- Why it matters. Solid tumours past about 1–2 mm cubed can’t grow any further without recruiting their own blood supply. Anti- angiogenic drugs (bevacizumab and family) are core oncology because cutting off that supply reliably slows tumour growth. The mirror concern is that adding angiogenic signal could feed pre-existing micro-tumours users don’t know about.
- What the evidence shows. No published cases of de novo cancer caused by short-cycle BPC-157 or TB-500 use. The concern is consistently framed as “could theoretically accelerate existing malignancies” rather than “causes cancer.” Animal models of BPC-157 do not show tumour induction at standard doses. Long-term human data is genuinely thin.
- Practical translation. Don’t run angiogenic peptides if you have an active cancer or recent (within ~5 years) cancer history. For everyone else, the cycling discipline (4–8 weeks on, equal washout, see Cycling Strategies) is the standard risk-hygiene response - not because the mechanism stops working at week 8, but because it caps cumulative angiogenic exposure.
2. Mitogenesis and cell survival
- What it is. Driving cells to divide and resisting programmed cell death (apoptosis). IGF-1 LR3 is the headliner here. Native IGF-1 does this physiologically; LR3 does it harder and longer because the >1000x reduced IGFBP affinity means the signal stays on.
- Why it matters. This is the mechanism with the most concrete epidemiology behind it. Higher endogenous IGF-1 in adulthood is associated with higher rates of several cancers (prostate, colorectal, breast, lung) in population studies. The association isn’t weak; it’s repeatedly replicated, though the absolute risk shift per unit IGF-1 in healthy adults is smaller than the relative-risk numbers in headlines suggest.
- What the evidence shows. Native IGF-1 epidemiology is what it is. LR3 specifically has no human safety trials - the risk extrapolates from the IGF-1-receptor pharmacology, not from controlled studies of the analogue. Animal models show disproportionate visceral organ growth at sustained doses, which is the “bubble gut” phenomenon visible in extreme-physique bodybuilders. The cancer-promotion risk is theoretical at typical 4-week-blast doses but plausible enough that responsible operators don’t run LR3 continuously.
- Practical translation. LR3 in particular: 4-week cycles maximum, equal washout, absolute contraindication with cancer history (active or in remission). The pulsatile GH-axis stack (Mod GRF + Ipamorelin) raises IGF-1 modestly and physiologically, which sits in a different risk frame than sustained supraphysiologic LR3 levels do.
3. Cell migration
- What it is. Promoting cell movement through tissue. TB-500’s active fragment is a cell-migration promoter, which is exactly the property that makes it useful for tendon and fascia repair - cells move into the injury site and begin remodelling.
- Why it matters. Metastasis is, mechanistically, cancer cells migrating from a primary site to a secondary location. A compound that promotes cell movement is at least conceptually compatible with that step.
- What the evidence shows. No documented cases of TB-500- induced metastasis. The mechanism is plausible but the magnitude of the effect on cancer cells specifically (versus the local fibroblasts and stem cells where Tβ4 acts) is unclear. The community standard treats the concern as real but doesn’t have a specific quantitative risk estimate.
- Practical translation. Same rule as the angiogenic class: don’t run TB-500 with active or recent cancer history. The 6–8-week-on / equal-washout pattern is the standard response. Pair-stacking with BPC-157 for healing protocols is fine in non-cancer-context users; the angiogenesis + migration combination is part of why that pair works for tendon repair, but it doubles down on the theoretical concern in users with malignancy risk.
What the evidence does not say
Honest framing of the limits matters here, because the catastrophising and the hand-waving both miss it.
- No published case series of healthy adults developing cancer from BPC-157, TB-500, IGF-1 LR3 or GHK-Cu use. Absence of evidence is not evidence of absence - the surveillance simply isn’t there for grey- market peptide use - but the operators who’ve been running these for a decade haven’t produced a flood of red-flag cases that the community has coalesced around.
- The IGF-1 epidemiology is on native IGF-1 levels in untreated populations. It does not directly translate to LR3-driven elevations, which are higher-magnitude and shorter-duration in typical use. The direction of risk is consistent with the data; the magnitude is extrapolation.
- Tumour-promotion risk is mechanism-plausible, not case-confirmed. “Could theoretically accelerate” is the correct frame. Anyone telling you these compounds “definitely cause cancer” is overstating what the data supports; anyone telling you they “have no cancer risk because there’s no proof” is dismissing a mechanism with concrete biology behind it.
Pre-cycle screen: what’s actually worth doing
Most of the screening value comes from one bloodwork session, one symptom review, and one age/family-history check. The screen below is the operator-grade minimum for anyone planning to run BPC/TB stacks, GH-axis or LR3 protocols.
Universal (every user)
- CBC with differential. Catches occult haematologic abnormality early. A persistently elevated white count, unexplained anaemia, or platelet abnormalities are signal to investigate before, not after, starting a peptide.
- CMP. Liver and kidney baseline; flags occult organ abnormality.
- Symptom review. Any unexplained weight loss, persistent night sweats, palpable lumps, persistent change in bowel or urinary habits, or blood where blood doesn’t belong - pause the protocol planning and investigate. These are the standard non-specific cancer symptoms; ignoring them so a peptide cycle can start on schedule is the wrong trade.
Age-appropriate cancer screening (don’t skip)
- Colonoscopy at the standard population age (45 in the US, 50 in many European systems - check local guidance) and on whatever cadence your last result drives.
- Skin survey - if you’re running MT-II or planning sustained sun exposure alongside any growth-factor peptide, a baseline dermatology check is proportionate. Photographic moles map matters more than a one-time visit over time.
- Prostate - PSA at age-appropriate cadence, especially relevant for IGF-1-elevating protocols given the IGF-1/prostate epidemiology.
- Breast / cervical - standard population screening. Don’t skip because peptides aren’t known to drive these specifically; the population-level risk is what it is.
Family history red flags
- First-degree relative with early-onset cancer (especially breast, ovarian, colorectal, or pancreatic before age 50) shifts the risk calculation. Weigh growth-factor protocols accordingly - this is exactly where the LR3-style aggressive anabolic signalling starts to look cost-disproportionate to a realistic body-comp goal.
- Known cancer-predisposition syndromes (Lynch, BRCA, Li-Fraumeni) put the angiogenic and growth-factor classes essentially off the table outside very short healing-only cycles.
Risk-tier decision framework
Combining the per-compound risk profile with the pre-cycle screen, three rough user tiers fall out.
- Low risk. No personal cancer history, no first-degree
relatives with early-onset disease, age-appropriate screening current, baseline
bloodwork normal, no current symptom red flags.
→ Standard cycling discipline applies. BPC/TB/GHK protocols, GH-axis protocols, occasional LR3 4-week blasts in AAS context all are reasonable with the standard cycle/washout pattern. Bracket each protocol with bloodwork as described in Bloodwork for Peptide Users. - Moderate risk. First-degree relatives with cancer history
(not early-onset), or age 50+ with screening current. No active or remission
history personally.
→ Angiogenic and healing peptides remain reasonable with stricter cycle discipline. LR3 specifically becomes harder to justify - the body-comp return is rarely large enough to outweigh the concrete risk-frame here. Pulsatile GH-axis (which produces modest physiologic IGF-1 elevation) is qualitatively different and remains an option. - High risk. Personal cancer history (active or in remission
within ~5 years), known cancer-predisposition syndrome, or current symptom red
flags.
→ Growth-factor and angiogenic peptides should be off the table. This is not the application class to solve a body-comp problem in. Recovery and quality-of-life peptides with negligible mitogenic profile (Thymosin Alpha-1, Selank, Semax) may still be reasonable; check with an oncologist familiar with the specific compound where possible.
What stops people
- Treating the question as binary. “Is BPC-157 safe, yes/no” isn’t the right question. The mechanism-plus-personal-risk frame produces useful answers; the binary frame doesn’t.
- Skipping pre-cycle bloodwork because nothing’s wrong. The point of the baseline isn’t to find current cancer. It’s to establish your normal, so that 6 months later you have a non-protocol-confounded reference if something does shift.
- Skipping age-appropriate screening because peptides aren’t known to drive that specific cancer. The population-level risk is what it is. Peptides don’t change baseline screening cadence either way.
- Running LR3 because “there’s no proof of harm.” Absence of human trials is not the same as absence of risk. The mechanism is well-characterised; the epidemiology of native IGF-1 elevation is consistent; the 4-week-blast cycling pattern is the community’s honest acknowledgement that continuous use is hard to justify.
- Stacking BPC-157 + TB-500 + IGF-1 LR3 + GH-axis + AAS year-round. The risk profile of each compound is small in isolation, larger together, and largest sustained. Stage compounds. The user who runs healing peptides during injuries, GH-axis through a cut, and IGF-1 in 4-week blasts has a manageable cumulative exposure. The user who runs all four continuously does not.
Cross-references
- Bloodwork for Peptide Users - the per-compound monitoring panel and timing.
- Peptides and Insulin - the metabolic-side question on the same axis: GH/IGF-1-driven insulin resistance over a cycle, when HOMA-IR or CGM start earning their keep.
- Cycling Strategies - the on/off rationale that maps to the risk-hygiene framing here.
- Sourcing and Verification - counterfeit peptides shift the risk picture in unpredictable ways.
- Lean Mass and Hypertrophy application - for the dose-strategy and risk framing of LR3 and the GH axis specifically.
- Injury Recovery application - for the BPC-157 / TB-500 healing protocols.