The single most common failure mode on GLP-1 weight loss is not nausea, not stalled scale weight, and not a side-effect that lands someone in a clinic. It’s a body that weighs less but looks worse - same waist, weaker lifts, flatter delts, softer arms. Pure scale weight came down. Lean mass came down with it.
This article puts numbers on how much muscle the trials actually saw lost, separates the fixable causes from the unfixable ones, and lays out the protein, training, and adjunct levers that change the outcome.
What the trials actually measured
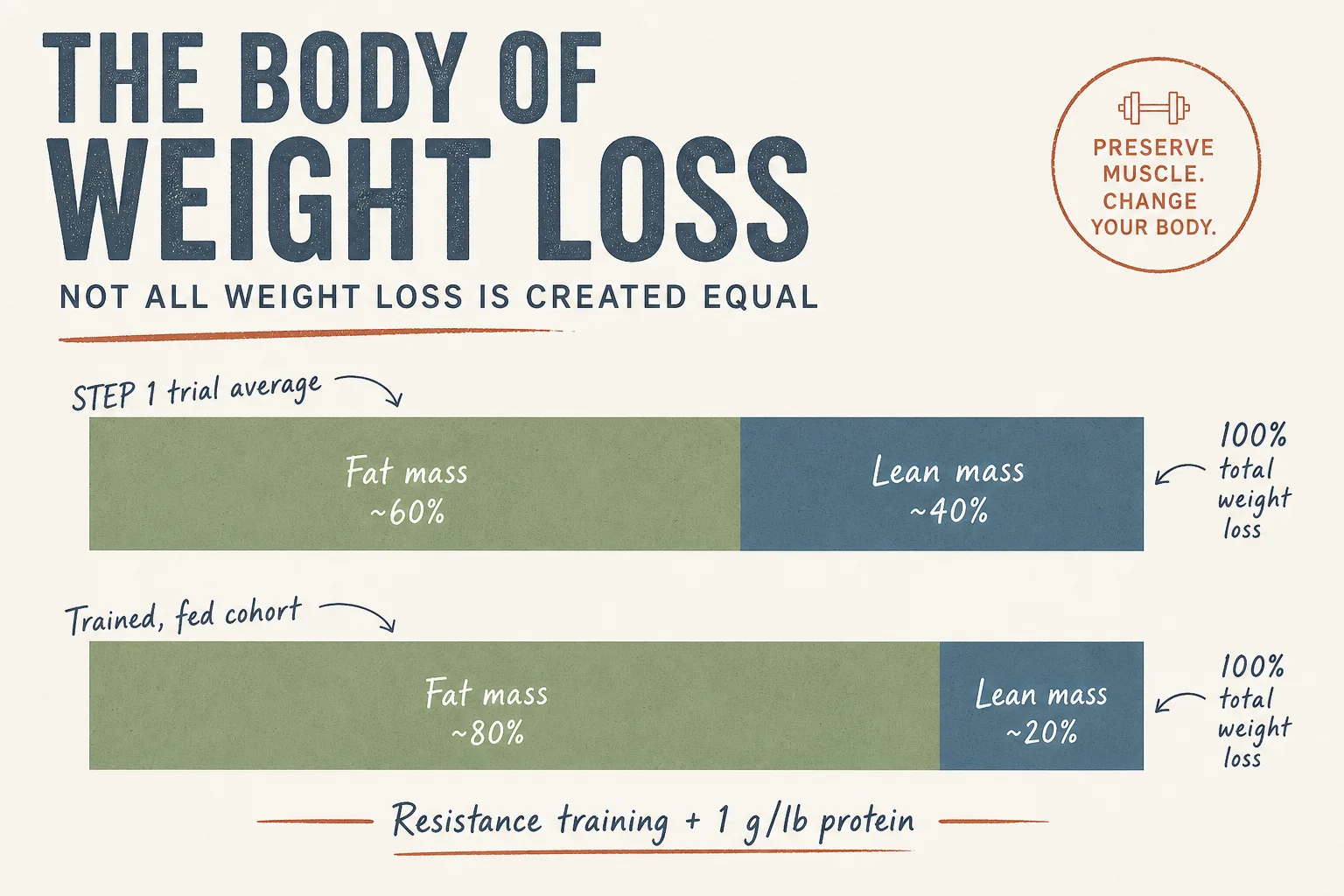
Both pivotal trials used DEXA sub-studies to break weight loss into fat mass and lean mass. Top-line numbers, rounded to the nearest percent:
- STEP 1 sub-study (semaglutide 2.4 mg, 68 weeks). Total weight loss ~14.9%. Of that, roughly 40% came from lean body mass and ~60% from fat mass. In absolute terms: a 100 kg participant losing ~15 kg of body weight lost roughly 6 kg of lean tissue and 9 kg of fat.
- SURMOUNT-1 sub-study (tirzepatide 5/10/15 mg, 72 weeks). Total weight loss ~20.9% on the high dose. Lean-mass fraction was similar in shape - ~25–33% of total weight loss across dose arms came from lean mass, depending on how you slice the DEXA cohort.
Two things matter about those numbers. First: they are averages of trial populations who were not asked to lift weights or hit specific protein targets. Resistance training was not a protocol requirement. Protein intake was not enforced. The trial participant who is sedentary and eats whatever appetite suppression allows is the default in those numbers.
Second: the fraction of weight loss coming from lean mass is roughly what you see in any energy deficit without resistance training and adequate protein. GLP-1s are not uniquely catabolic. They are uniquely effective at producing the deficit, and the deficit does the rest.
Why the lean-mass loss happens
In rough order of contribution:
- Aggressive deficit without protein. Strong appetite suppression drops calorie intake by 20–40% within weeks. Protein, the most satiating macronutrient, drops alongside total intake unless it’s deliberately preserved. A protein deficit on top of an energy deficit is the textbook recipe for net negative nitrogen balance.
- No resistance-training stimulus. Muscle that isn’t loaded isn’t being told it’s needed. In a deficit, the body settles disputes about what to keep by looking at recent demand.
- Rapid titration. Climbing the dose every two weeks instead of every four amplifies appetite suppression before behaviour can adjust. The first 8–12 weeks at maximum tolerable dose are when most of the lean-mass damage happens.
- Underdosed sleep, low NEAT. GLP-1 users often spontaneously sit more, walk less, and sleep worse during titration. Lean-mass preservation is a recovery problem; recovery is a sleep-and-NEAT problem.
Note what isn’t on this list: a direct catabolic action of GLP-1 on muscle tissue. The receptor density story doesn’t support a special “GLP-1 melts muscle” mechanism. The mechanism is the deficit, applied harder than most users have ever applied one before.
The four levers that change the outcome
1. Protein at 1 g per lb of goal body weight
Not current body weight - goal body weight. For a 220 lb user aiming for 180 lb, that’s 180 g/day, every day. On hard appetite suppression weeks, this is the hardest part of the protocol. Practical patterns that work:
- Two 50–60 g protein meals as non-negotiable anchors, scheduled before nausea windows (typically morning and early afternoon for once-weekly dosing).
- Whey or casein shake as a third anchor when solid food is unappealing. Liquid protein bypasses most of the appetite-suppression friction.
- Lean meat, Greek yoghurt, eggs, cottage cheese as the rotation. Avoid front-loading fibrous vegetables and mixed-macro meals on injection day - gastric emptying is already slow.
2. Resistance training, 3+ sessions per week, progressive load
Not cardio. Not Pilates. Not “walking 10k steps”. Those are fine adjuncts but they don’t generate the muscle-preservation signal that matters here. The minimum effective protocol is a full-body or upper/lower split with the four compound patterns - squat, hinge, push, pull - loaded heavy enough to be hard for 5–8 reps, 2–4 working sets per pattern per week.
The signal is the load, not the calorie burn. A 30-minute session with three heavy sets per movement does more for lean-mass preservation than a 60-minute high-rep circuit.
3. Slower titration than the package insert
The Wegovy / Zepbound / off-label titration schedules climb dose every four weeks. That is the floor, not the target. Holding at each step for 6–8 weeks before climbing - and stopping the climb at the lowest dose that produces steady weekly fat loss - trades a few weeks of timeline for substantially better body-composition outcomes. Per-compound step-up tables and the slow-ramp variant in the GLP-1 Titration Schedule.
Practical rule: if scale weight is dropping at 0.5–1% body weight per week and strength markers are holding, do not climb the dose. The dose only needs to go up when the deficit has stalled.
4. GH-axis adjuncts when the budget allows
The case for stacking Mod GRF 1-29 + Ipamorelin pre-bed alongside GLP-1 is not that they add fat-loss firepower - they don’t, meaningfully. The case is that they improve sleep quality and recovery on a deficit, both of which feed back into training performance and lean-mass retention. The cost-to-benefit is favourable; the side-effect surface is small.
CJC-1295 (DAC) for continuous IGF-1 elevation is a more aggressive option with a stronger anabolic-signalling case but more downstream monitoring required. See GH Axis Playbook for the trade-offs.
What about IGF-1 LR3 or PEG-MGF for direct anabolic support? They have a real mechanism but a much wider risk profile, and they introduce questions GLP-1 users don’t need on top of an already busy protocol. Reserve them for users who already have AAS context and know how to monitor.
What “preserved” looks like in numbers
A trained user running the four levers above, on tirzepatide for a 20% cut over six months, can reasonably expect:
- Lean-mass fraction of total loss: 10–20% rather than 25–40%.
- Working-set strength: held within ~5% of baseline at end of cut, fully recovered or exceeded after a 4–6 week post-cut maintenance phase.
- DEXA or skin-fold body-fat percentage: dropping ~1 percentage point per month on average, slower in the final 5%.
Untrained users running the same compound without the four levers will see a 30–40% lean-mass fraction of loss, scale weight that drops fast in the first three months and stalls early, and a body that looks softer at the lower weight than the higher weight. Same compound, different outcome.
Monitoring: what tells you it’s working
- Working-set load on 3–4 key lifts. Squat, deadlift, bench, overhead press. Track them weekly. Drift downward on these is the muscle-loss alarm that fires before a DEXA picks it up.
- Waist circumference and a chest/arm/thigh tape measure. Weekly. Waist down + arms down at the same rate is fat loss going well. Waist down + arms down faster than waist is bad ratio.
- Photos. Day zero and monthly, same lighting, same poses. Memory of starting condition gets unreliable on a successful cut; photos don’t.
- DEXA at baseline and end-of-cut. Optional but ideal. The number that matters is lean-mass-loss-as-fraction-of-total, not absolute lean-mass change.
- Bloodwork. See Bloodwork for Peptide Users for the full panel. For this protocol specifically: HbA1c, fasting glucose, lipids, CBC, IGF-1 if running a GH-axis adjunct.
What stops people from getting this right
- Treating protein as a target, not a floor. 180 g is the floor on a cut day, not the goal. Hitting 150 four days a week and 200 the other three averages fine on paper and fails in practice.
- Skipping training on injection day. The 24–48 hours after a once-weekly injection are when nausea peaks. They’re also when most users spontaneously skip the gym. Move training to days 4–6 post-injection by default.
- Climbing dose for the sake of climbing. Many users follow the package-insert schedule on autopilot and end up at 15 mg tirzepatide when 7.5 mg was producing the same loss rate with half the muscle-mass cost.
- Confusing scale weight with progress. Hydration shifts on GLP-1 early, glycogen drops with carb intake, and bowel-movement-frequency changes mask the underlying fat-loss curve. Weekly waist + strength + photos is the real signal.
- Stopping cold without a maintenance protocol. The rebound on these compounds is well-documented. A taper plan from week one matters; so does the protein and training maintenance protocol after.
Cross-references
- Fat Loss application - the broader decision tree across families.
- Semaglutide vs Tirzepatide vs Retatrutide - per-compound choice.
- GH Axis Playbook - for the adjunct stacking decision.
- Bloodwork for Peptide Users - monitoring panel and cadence.