This is the application where evidence quality drops fastest. The fat-loss compounds on this site (GLP-1 family, tesamorelin) ship with phase 3 data. The lean-mass compounds mostly don’t. Honest framing of what each compound actually has behind it - and where the line is between “animal models say it should work” and “humans on it say it does work” - matters more here than anywhere else in the catalogue.
The audience for this page is already running training, nutrition, sleep, and (in many cases) AAS. Peptides are the marginal lever, not the foundation. With that frame: the lean-mass shortlist sorts cleanly by evidence tier, and the higher-leverage compounds carry the higher monitoring burden.
The compounds, sorted by what we actually know
Tier 1 - clinical-grade evidence
- Somatropin (rHGH). Decades of clinical use for adult and paediatric GH deficiency, well-characterised side-effect profile, FDA-approved with multiple branded products. The strongest body-composition signal available. The cost is the monitoring burden - HbA1c drift, fluid retention, carpal-tunnel-like symptoms at higher doses, IGF-1 elevation that needs bracketing - and the cost is genuinely the cost.
Tier 2 - mechanism-of-action and pulsatile-GH evidence
- Mod GRF 1-29 + Ipamorelin. Pulsatile GHRH + GHRP architecture. The mechanism is well-characterised, the GH pulse is real and measurable on bloodwork, the IGF-1 elevation is modest and physiologic. The pure hypertrophy effect is also modest - this stack is recovery and sleep infrastructure first, lean-mass infrastructure second. Pair with the actual training stimulus rather than expecting it to drive growth on its own.
- CJC-1295 (DAC). Continuous IGF-1 elevation rather than pulsatile. More water retention, more insulin-sensitivity drift risk; the lean-mass return relative to those costs is the worst in the GH-axis family. Use only when the convenience of weekly dosing is genuinely load-bearing.
Tier 3 - animal data plus community logs
- IGF-1 LR3. No published human trials for the LR3 analogue specifically; clinical IGF-1 data is on rhIGF-1 (Mecasermin), a different molecule. The mechanism is biologically sound - the LR3 modification reduces IGFBP affinity by >1000x, so it acts as a long-half-life “super-IGF-1” in animal models. Tomas et al. (1991) confirmed higher potency than rhIGF-1 in rats. Community logs are extensive but noisy because the counterfeit rate is high.
- PEG-MGF. Pegylated synthetic MGF (mechano growth factor, IGF-1Ec splice variant). Goldspink’s preclinical work is the cleanest source on the satellite-cell-activation mechanism, but no human trials of the pegylated peptide exist. Community use centres on lagging body parts with local injection. Outcomes are highly variable; counterfeit rate is significant.
Tier 4 - high uncertainty, structural risks
- Follistatin-344. The Becker muscular dystrophy gene-therapy work used AAV1-follistatin gene transfer, NOT the peptide grey-market users inject. Animal data on follistatin overexpression is genuinely impressive (the “double-muscling” phenotype). Translation to a stable injectable peptide in healthy adults is unproven. Counterfeit and instability rates are among the highest in the catalogue, and the structural-risk story (tendon ratio mismatched to muscle hypertrophy, cardiac concerns) is real enough that experienced users treat this as an experimental compound, not a routine one.
- IGF-1 DES. Specialist site-enhancement use case with very short half-life and fiddly local-injection logistics. Niche.
Decision guide
- Have you actually exhausted the training, nutrition, sleep, and recovery
levers?
→ If the protein floor is below 1 g per lb of goal body weight, sleep is irregular, or training programming is unfocused, no compound on this list will rescue that. Peptides are the marginal lever; they do not build a foundation that isn’t there. - Are you running AAS?
→ Yes → the GH-axis stack (Mod GRF + Ipa pulsatile, optionally CJC-DAC for continuous) is the natural pairing. AAS provides the testosterone-driven anabolic signal; the GH axis adds recovery and IGF-1 leverage. IGF-1 LR3 in short blasts sits on top for advanced operators who already monitor closely.
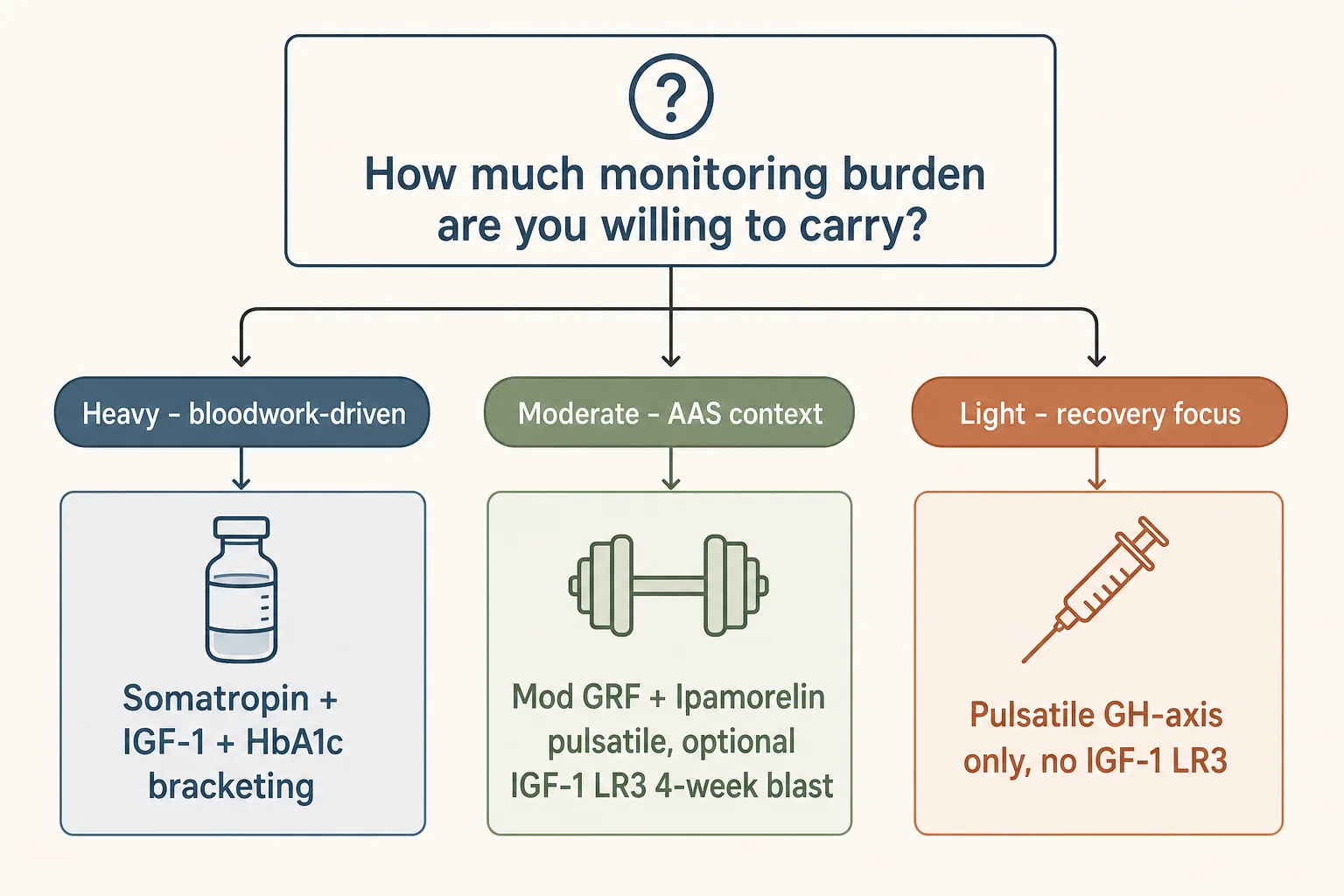
→ No → honest answer: peptides alone produce a meaningfully smaller body- comp shift than peptides + AAS. The pulsatile stack is still worth running for recovery and sleep benefit; expect modest hypertrophy returns. - How much monitoring burden are you willing to carry?
→ Heavy → somatropin + bloodwork-driven titration. Strongest signal, requires the discipline.
→ Moderate → pulsatile GH-axis (Mod GRF + Ipamorelin), optional IGF-1 LR3 blast in the front of an AAS cycle.
→ Light → just the GH-axis stack, no IGF-1 LR3, no follistatin. - Are growth-pathway risks something you weigh heavily?
→ Yes → skip IGF-1 LR3 entirely and de-prioritise CJC-DAC. Pulsatile GH-axis raises IGF-1 modestly and physiologically; sustained supraphysiologic IGF-1 is the part of this protocol with the most concrete long-term concern. - Tested athlete (WADA / USADA / league)?
→ All of this is S2. None of it is compatible with tested competition without a TUE pathway.
Representative stacks
Stack 1 - Pulsatile GH-axis (lowest burden, broadest fit)
- Mod GRF 1-29 100 mcg + Ipamorelin 200 mcg pre-bed, daily
- Optional second pulse: same combination post-workout on training days
- 5 days on / 2 days off pattern after the first 8 weeks if IGF-1 has stalled (see Cycling Strategies)
- Run for 6–12 months; expect recovery and sleep returns first, lean-mass returns second
- Bloodwork: IGF-1 baseline + 6 weeks then quarterly; HbA1c, fasting glucose, lipids quarterly (see Bloodwork for Peptide Users)
Stack 2 - AAS-context hypertrophy blast (advanced operators only)
- IGF-1 LR3 30–50 mcg subcutaneous post- workout, 4 weeks maximum, with a minimum 4-week washout before repeating
- Carbohydrates immediately post-injection (30–50 g fast carbs) - non-negotiable. The hypoglycemia risk is real and acute. Never stack with exogenous insulin; see the Stacking Safety Quick Reference for the full conflict list.
- Stacked underneath the AAS testosterone backbone, alongside Stack 1’s pulsatile GH-axis support
- Bloodwork: IGF-1, HbA1c, fasting glucose, CBC, lipids at baseline + week 4 + post- washout; full-spectrum lipids and hematocrit on standard AAS-cycle cadence
- Source verification before trusting bloodwork interpretation - the IGF-1 response confirms the compound is real (see Sourcing and Verification)
Stack 3 - Somatropin protocol (highest leverage, highest burden)
- Somatropin 2–4 IU/day subcutaneous, titrated against IGF-1 (target generally 200–300 ng/mL for hypertrophy contexts - lab-specific reference ranges vary)
- Pre-bed dosing or split AM/PM; on an empty stomach
- Run continuously for 4–8 months at minimum; below that horizon the body-comp return doesn’t justify the cost
- Bloodwork: IGF-1 baseline + monthly for the first quarter, then every 6–8 weeks; HbA1c and fasting glucose every 8 weeks; lipids and CBC quarterly
- Stop if HbA1c climbs into pre-diabetic range and doesn’t recover with dose reduction
What stops people
- Treating LR3 like a routine compound. The combination of acute hypoglycemia risk, no human trials, and a counterfeit market that’s near the worst in the catalogue makes this a 4-week blast tool, not a daily multivitamin. Operators who run it month after month have the worst long-tail outcomes in the application.
- Skipping the carbs after IGF-1 injection. The most concrete immediate-risk failure mode in this entire application. Coma is on the table for untreated severe hypoglycemia. This is non-negotiable, not optional.
- Buying counterfeit follistatin. The peptide is structurally unstable and the manufacturing demands are real. Most of what users inject is not biologically active follistatin. Bloodwork can’t easily verify it because the expected anabolic signal is confounded by training and AAS.
- Stacking too many anabolic signals at once. AAS + GH + IGF-1 LR3 + follistatin is the classic “everything everywhere all at once” mistake. The risk profile multiplies; the lean-mass return doesn’t. Stage compounds rather than stacking them.
- Ignoring HbA1c drift. GH-axis manipulation, especially with somatropin or sustained IGF-1 elevation, pushes insulin sensitivity downward over months. The user who catches HbA1c climbing in week 8 adjusts dose; the user who measures only at month 6 has months of compounded metabolic damage.
- Stopping cold without keeping the foundation. Lean mass added during a peptide protocol stays in proportion to what training and protein discipline justify post-protocol. Drop both, and the compounded gains drop with them.
Monitoring on this protocol
- IGF-1. The primary “is the protocol working” lab. Baseline + 6 weeks for any GH-axis or IGF-1 protocol; more often during titration.
- HbA1c, fasting glucose. Every 8 weeks. The single most important safety lab for this application class.
- Lipids, CBC, hematocrit. Quarterly, more often if AAS is in the mix.
- Working-set strength on 4–6 key compound lifts. Tracked weekly. The cleanest non-bloodwork signal that the protocol is producing the intended adaptation rather than just water retention.
- Body composition. Skinfolds or DEXA quarterly. Resist the urge to measure scale weight as the primary metric - water retention shifts from GH-axis manipulation can mislead by 2–4 kg either direction.
- Photographs. Day zero plus monthly. Same lighting, same poses. Visible change in delts, arms, mid-back lats. See GLP-1 and Muscle Preservation for the parallel discipline on the cutting side - the principle that photos-plus-strength tells you more than scale-weight is the same here.
Cross-references
- GH Axis Playbook - pulsatile vs continuous decision in detail.
- Cycling Strategies - especially for the LR3 4-week-blast pattern.
- Bloodwork for Peptide Users - the per-compound monitoring panel and cadence.
- Sourcing and Verification - particularly load-bearing for IGF-1 LR3 and follistatin where the counterfeit rate is highest.
- Fat Loss application - for the cut-side mirror of this protocol set.
- Injury Recovery application - BPC/TB stacking that pairs well with hypertrophy work.