Fat loss in 2026 is a different conversation than it was five years ago. The GLP-1 family has changed the ceiling of what’s possible without surgery, and the older fat-loss peptides - AOD-9604, Fragment 176-191, GH-axis stacks - have moved into supporting roles. This page sorts the families by what they actually do, then picks between them by goal, budget, side-effect tolerance, and whether you’re running anabolics alongside.
The honest framing: the audience this site is written for almost always wants a deeper cut than the diet alone produces, and a faster timeline than walking-and-protein delivers. The peptides earn their place when they shorten that cut and protect what was built. They don’t replace the deficit, the protein, or the training.
The three families
GLP-1 family - the modern frontline
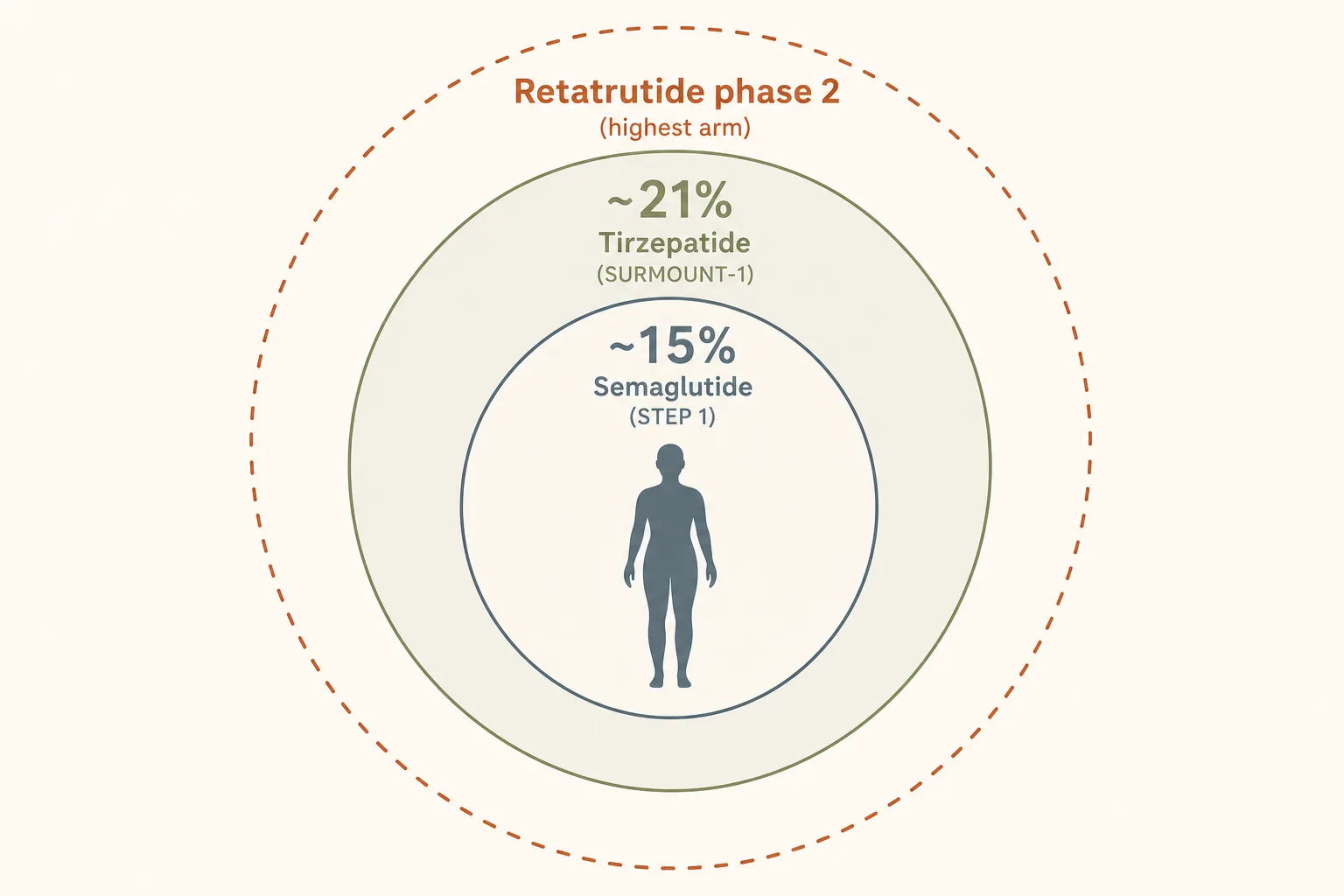
- What they are: incretin-receptor agonists. Semaglutide hits GLP-1. Tirzepatide hits GLP-1 + GIP. Retatrutide hits GLP-1 + GIP + glucagon.
- What they do: crush food noise, slow gastric emptying, and (retatrutide) raise energy expenditure. Phase 3 weight-loss numbers are roughly 15% on semaglutide, 21% on tirzepatide, and higher on retatrutide’s phase-2 high-dose arm.
- Cost reality: approved channels (Wegovy, Zepbound, prescription semaglutide/tirzepatide) are expensive without insurance, but the verification problem is solved - the vial contains what the label says. Grey-market routes are cheaper but bring source-quality risk; see Sourcing and Verification.
- The trade-off: appetite suppression is the mechanism. That means muscle loss is the failure mode if protein and resistance training don’t hold the line. Anyone running these without resistance training and 1 g protein per lb of goal body weight is, by default, losing both fat and muscle at roughly the same rate weight-loss-trial averages show.
- Per-compound choice: see Semaglutide vs Tirzepatide vs Retatrutide. Short version: semaglutide first if you want the most-studied option, tirzepatide if you need the higher ceiling, retatrutide only if both have failed and source quality can be controlled.
- Oral options: Rybelsus (oral semaglutide via SNAC absorption enhancer) and Orforglipron (Lilly small-molecule GLP-1 RA, expected approval 2026) reshape who actually needs the injectable. Worth reading before starting if a pill is logistically easier - The Oral GLP-1 Era.
GH axis - the supporting infrastructure
- What it is: pulsatile Mod GRF 1-29 + Ipamorelin, or in some cases CJC-1295 (DAC) for continuous IGF-1 elevation. Tesamorelin for visceral fat specifically (it has direct human VAT data).
- What it does for fat loss: mild lipolysis, better recovery on a deficit, modestly better sleep. Not a primary fat-loss tool when GLP-1 is on the table; a meaningful adjunct when it isn’t, or alongside one for muscle preservation benefits.
- The visceral-fat case: Tesamorelin has direct human-trial data for visceral adipose tissue reduction in HIV-lipodystrophy and is the cleanest mechanism for that specific compartment. If visceral fat is the primary goal rather than a sub-case of overall fat loss, the dedicated Visceral Fat application has the full decision tree, stacks and monitoring plan; see also GH Axis Playbook for the pulsatile-vs- continuous comparison.
- Cost reality: Mod GRF + Ipamorelin is among the cheapest peptide stacks in the catalog. Tesamorelin is approved (Egrifta) but pharmacy pricing is steep; grey-market is the common route.
HGH fragments - niche, mostly historical
- What they are: AOD-9604 and Fragment 176-191 isolate the C-terminal, lipolytic part of HGH and discard the IGF-1-mediated anabolic and insulin-desensitizing parts.
- What they actually do: mild lipolysis without water retention or insulin disturbance. Theoretically attractive. The clinical-trial reality, though, is that AOD-9604 failed to beat placebo at the obesity endpoint - the development program was abandoned. Fragment 176-191 has no real human trial data of its own.
- Where they fit now: stubborn-fat protocols in fasted-cardio windows where the user wants a lipolytic nudge without affecting bloodwork or appetite. Useful in AAS contexts where GLP-1 nausea is a problem and GH-axis isn’t enough. Outside those niches, GLP-1 just outperforms.
- WADA flag: AOD-9604 is on S0 (non-approved substances). Fragment 176-191 is on S2. Tested athletes should treat both as off-limits.
Decision guide
- Have you exhausted training-and-nutrition adjustments first?
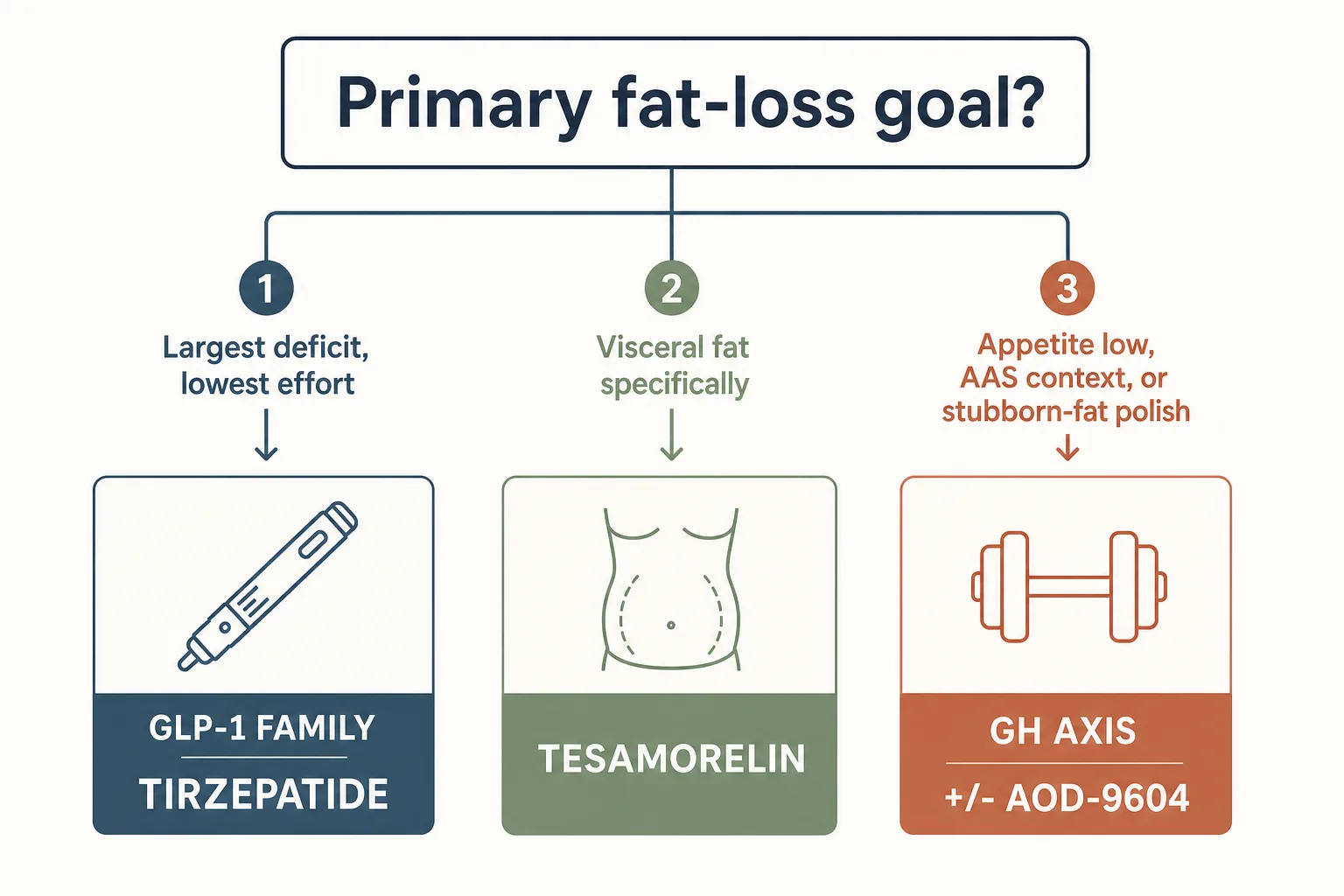
→ If not, fix that first. Peptides accelerate the right curve; they don’t bend a wrong one. - Do you want the largest possible deficit at the lowest possible
effort?
→ Tirzepatide via approved channel if accessible, Semaglutide if not. Plan the muscle-preservation protocol before starting. - Is the goal specifically visceral fat reduction (not subcutaneous)?
→ Tesamorelin. The human VAT data is unique to this compound. GLP-1 still helps subcutaneously alongside. - Is appetite already low and the limiter is recovery / sleep / lipolysis at
the margin?
→ Mod GRF + Ipamorelin pre-bed. Cheap, clean, low side-effect surface. - Are you running AAS and don’t want appetite suppression?
→ GH axis as primary fat-loss support, with optional AOD-9604 in fasted-cardio window if stubborn-fat is the issue. GLP-1 stacks awkwardly with eating-to-grow goals and is usually not the right tool when AAS-driven appetite is itself the asset. - Tested athlete (WADA, USADA, league)?
→ All of GH axis, GLP-1, and HGH fragments are subject to bans (S2 / S0 / S2 respectively). Verify TUE pathway and current league rules before any of this.
Representative stacks
Stack 1 - First-line cut, no AAS
- Tirzepatide 2.5 mg weekly, titrating up by 2.5 mg every 4 weeks, hold at the lowest effective dose
- Optional: Mod GRF 100 mcg + Ipamorelin 200 mcg pre-bed for sleep / recovery benefit; not load-bearing for the cut
- Protein at 1 g per lb of goal body weight; 3+ resistance training sessions/week with progressive overload
- Bloodwork: HbA1c, fasting glucose, lipids, CBC at baseline + 8 weeks (see Bloodwork for Peptide Users)
Stack 2 - AAS context, appetite is an asset
- Mod GRF 100 mcg + Ipamorelin 200 mcg, twice daily (pre-bed + post-workout)
- Optional: AOD-9604 300 mcg pre-fasted-cardio, 3–5x/week, for stubborn-fat targeting
- No GLP-1 in this configuration unless the user explicitly wants the appetite suppression
- Bloodwork: IGF-1 baseline + 6 weeks; lipids and hematocrit (especially with AAS) on standard cycle cadence
Stack 3 - Visceral-fat focus
Quick version below; the dedicated Visceral Fat application is the deeper read with the imaging-first monitoring plan.
- Tesamorelin 1 mg subcutaneous daily for 12–26 weeks (clinical-protocol range)
- Optional: low-dose Semaglutide alongside if subcutaneous fat is also a target; doesn’t conflict mechanistically
- VAT measurement (DEXA or imaging) at baseline and at 12 weeks - this is the application where measuring the right compartment matters most, since scale weight moves slowly on tesamorelin alone
- Bloodwork: IGF-1 baseline + 6 weeks; HbA1c every 12 weeks
What stops people
- Muscle loss on GLP-1. The single most common failure. Hard appetite suppression + no resistance-training discipline = lean-mass loss roughly proportional to fat loss. Treat protein and training as non-negotiables, not options. Full numbers, titration nuance, and the four levers that change the outcome: GLP-1 and Muscle Preservation.
- Titrating too fast. The package insert schedule is the floor, not the target. Climbing dose every two weeks instead of every four trades a few weeks of timeline for severe nausea, vomiting, and an early discontinuation.
- Stopping cold. The rebound on GLP-1 family compounds is real and well-documented. A taper plan from week one matters; so does the maintenance protocol after.
- Mistaking AOD/Fragment for a primary tool. They didn’t beat placebo in the trials they were designed for. They have a niche use; treating them as standalone fat-loss agents wastes a cycle and the budget.
- Source quality. Underdosed grey-market GLP-1s look like “non-responder” biology. Test before you blame the compound; see Sourcing and Verification.
- Bloodwork-blindness. HbA1c, lipids, IGF-1, and resting heart rate answer most of the “is this working / is this still safe” questions. Skipping them is the easiest way to wander into a problem you would’ve caught at week 8.
Monitoring on this protocol
- Body composition over scale weight. Track waist, hip, and a few skin-fold sites weekly. Scale alone misleads on GLP-1 because hydration shifts early.
- Strength markers. A working set in 3–4 key lifts (squat, deadlift, bench, OHP). Drift downward on these is the muscle-loss alarm.
- Resting heart rate. Especially on retatrutide; an 8–10+ bpm increase warrants a dose re-think.
- Bloodwork: see Bloodwork for Peptide Users for the per-class panel and timing.
- Photographic documentation. Day-zero photo plus monthly. Memory of starting condition gets unreliable fast on a successful cut; photos don’t.