Visceral adipose tissue (VAT) - the fat stored around the liver, pancreas, and intestines - is a different compartment than subcutaneous fat with a different metabolic risk profile and a different response to most fat-loss tools. The peptide shortlist for this goal is short, and the order matters more than for almost any other application on this site: only one peptide in the catalog has direct human VAT trial data.
This page treats Tesamorelin as primary by default, the broader GH-axis as a secondary lever for users who can’t access or afford tesamorelin, and a low-dose GLP-1 overlay as the optional companion when subcutaneous fat is also a target. Everything else (AOD-9604, Fragment 176-191) is a fasted-window adjunct, not a primary tool.
Why VAT is its own problem
- Different metabolic signature. VAT drives more of the cardiometabolic risk picture than subcutaneous fat at the same total weight: insulin resistance, fatty-liver disease, dyslipidemia, and the inflammation that links abdominal obesity to long-term outcomes track VAT, not BMI.
- Different mobilisation. VAT is more lipolytically active than subcutaneous fat - it responds to catecholamines and to GH faster - but it also accumulates faster when GH and IGF-1 fall with age. The window where intervention shifts the visceral-to-subcutaneous ratio is real.
- Scale weight is a bad signal. A measurable VAT reduction can land while bodyweight barely moves, especially in users who are not in a substantial caloric deficit. Waist circumference moves earlier than weight; DEXA or imaging moves earliest of all.
The shortlist by role
Primary - Tesamorelin
- Mechanism. A stabilised GHRH analogue that drives endogenous pulsatile GH release. Selective VAT reduction is the unique part - a feature that other GH-axis agents share in part, but with substantially weaker direct evidence in the visceral compartment.
- Evidence. Phase III trials in HIV-associated lipodystrophy (Egrifta, Falutz 2010) showed VAT decreases of roughly 15–20% over 26 weeks at 2 mg/day vs placebo. Waist circumference shifted measurably. The trial population is HIV-positive lipodystrophy, so generalisation to healthy adults is extrapolation - but the mechanism is consistent and the real-world data from anti-aging clinics is consistent with the trials.
- Protocol. 2 mg subcutaneous once daily, before bed or fasted morning, on an empty stomach (insulin blunts GH release). 26 weeks is the trial duration; long-term clinical use runs 6–12 months. Many cost-conscious users drop to 1 mg/day with somewhat slower outcomes.
- Cycling. Trial data showed VAT returned after cessation, so a discontinuation strategy matters. Most users either run continuous through a goal cut, or use the 5-on/2-off pulse pattern shared with other GHRH agents (see Cycling Strategies).
- Cost reality. The largest barrier in this category. Pharmacy Egrifta is steeply priced; grey-market tesamorelin is the more common route, with the verification problem that attaches to all grey-market peptides - see Sourcing and Verification.
Secondary - GH-axis support
When tesamorelin is not accessible, the broader GH-axis still produces a meaningful shift, just with less specificity to the visceral compartment.
- Mod GRF 1-29 + Ipamorelin (pulsatile). Pre-bed plus optional second dose post-workout. The pulsatile architecture protects receptor sensitivity better than DAC variants and produces a cleaner IGF-1 curve. Cheaper than tesamorelin by an order of magnitude, fewer concerns about insulin sensitivity.
- CJC-1295 (DAC) (continuous). The convenience option - weekly or twice-weekly. Continuous IGF-1 elevation rather than pulsatile, which is a tradeoff: more sustained signal, more risk of insulin sensitivity drift, more tendency to retain water. Less the right tool than Mod GRF + Ipa for a body-comp goal where insulin markers matter.
- Somatropin (rHGH). The most direct GH signal in the catalog and the one with the highest monitoring burden. Effective for body composition, but for visceral fat specifically the literature favours pulsatile GHRH analogues over exogenous GH because the latter raises fasting glucose and HbA1c more reliably. Reserve for users with broader anti-aging goals already in scope.
Companion - GLP-1 overlay (optional)
Semaglutide or Tirzepatide at the low end of the dose range can sit alongside tesamorelin without conflict. The two work on different fat compartments - GLP-1 produces a generalised deficit that pulls subcutaneous fat first; tesamorelin selectively pulls VAT. A combined protocol is reasonable when the user has subcutaneous fat to lose and visceral fat as a specific concern, with the muscle- preservation discipline from GLP-1 and Muscle Preservation applied.
Tertiary - lipolytic adjuncts
- AOD-9604 and Fragment 176-191 in the fasted cardio window. Mild lipolytic effect, neutral for insulin and IGF-1, no real human VAT data of their own. They are not load-bearing for visceral-fat protocols. Useful only when a user wants a small additional lipolytic nudge in a fasted morning session and doesn’t want it to perturb appetite or glucose.
Decision guide
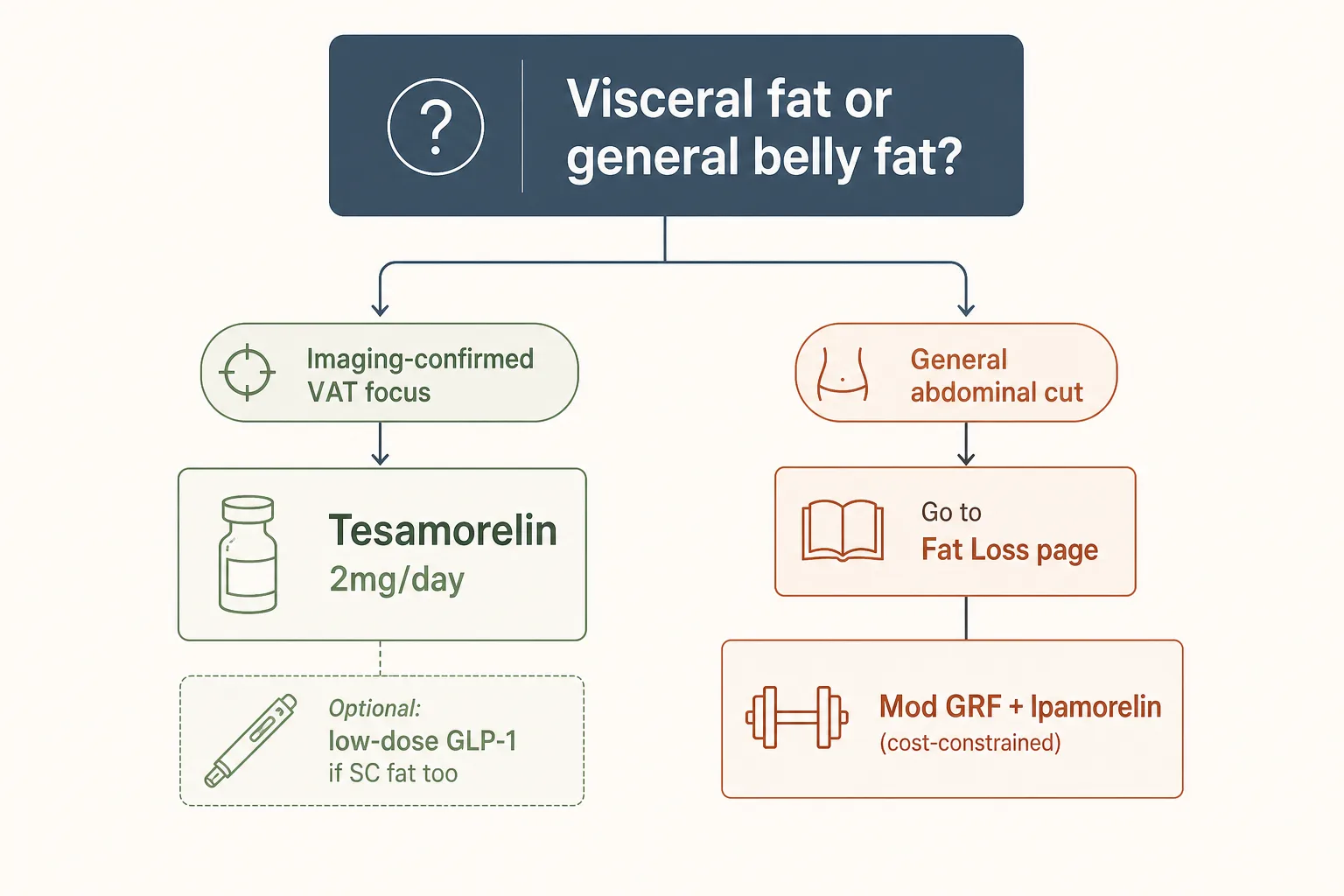
- Is the goal specifically visceral, or is it “abdominal fat”
in general?
→ If imaging confirms high VAT and subcutaneous is normal, tesamorelin first. If the user is just “trying to lose belly fat” without imaging, the answer is more likely the broader cut tools (see Fat Loss). - Can you access tesamorelin (cost, supply)?
→ Yes → tesamorelin 2 mg/day for 12–26 weeks, optionally with low-dose GLP-1 if subcutaneous is also in play.
→ No → Mod GRF + Ipamorelin pulsatile stack as a 6–12-month protocol. Slower, less specific, much cheaper. - Are insulin/glucose markers already drifting?
→ Yes → Stay pulsatile (tesamorelin or Mod GRF + Ipa). Avoid CJC-DAC and avoid somatropin without the broader anti-aging context. - Is significant subcutaneous fat also present?
→ Yes → Add a low-dose GLP-1 to the protocol. Don’t escalate the GLP-1 chasing scale weight - the visceral piece responds to the GH-axis lever, not the deficit. - Tested athlete (WADA / USADA)?
→ Tesamorelin and all GH-axis agents are S2. AOD/Fragment is S0 / S2. None of this is compatible with tested competition without a TUE pathway.
Representative stacks
Stack 1 - Visceral cut, tesamorelin primary
- Tesamorelin 2 mg subcutaneous daily, morning fasted or pre-bed, for 12–26 weeks
- Optional: Ipamorelin 100 mcg paired pre-bed for a tighter GH pulse
- Optional: low-dose Semaglutide 0.25–1 mg weekly if subcutaneous fat is also a target; do not chase scale weight
- VAT measurement (DEXA, MRI, or CT) at baseline and at 12 weeks
- Bloodwork: IGF-1 baseline + 6 weeks; HbA1c every 12 weeks; fasting glucose, lipids, CBC at baseline + 12 weeks (see Bloodwork for Peptide Users)
Stack 2 - Pulsatile GH-axis (cost-constrained)
- Mod GRF 1-29 100 mcg + Ipamorelin 200 mcg pre-bed, daily
- Optional second pulse: same combination post-workout on training days
- 5 days on / 2 days off pattern after the first 8 weeks if IGF-1 is climbing
- Run for 6–12 months; expect slower visceral shifts than tesamorelin
- Bloodwork: IGF-1 baseline + 6 weeks then quarterly; HbA1c, fasting glucose, lipids quarterly
Stack 3 - Combined visceral + subcutaneous focus
- Tesamorelin 2 mg/day for the visceral lever
- Tirzepatide 2.5 mg weekly, titrating slowly, held at the lowest dose producing 0.5–1% body-weight loss per week
- Protein at 1 g per lb of goal body weight; resistance training 3+ sessions/week (the muscle-preservation cost of GLP-1 is real - see that article)
- VAT measurement at baseline and 12 weeks; full body comp via DEXA quarterly
- Bloodwork: IGF-1, HbA1c, fasting glucose, lipids at baseline + 8 weeks + 16 weeks
What stops people
- Treating VAT and subcutaneous fat as the same problem. A user with low subcutaneous and high VAT often gets thrown a GLP-1 first because that’s the loudest tool. The GLP-1 will lose subcutaneous fat the user doesn’t have to spare and barely move VAT. Match the lever to the compartment.
- Skipping the imaging. Without DEXA or MRI, “visceral fat focus” is just “belly fat focus.” Imaging once is cheap relative to a 12-week tesamorelin protocol; not getting it means flying blind on the metric that matters most for this goal.
- Insulin sensitivity drift. Tesamorelin and GH-axis agents can shift HbA1c slightly upward, especially at higher doses or with CJC-DAC. Catching it early means you adjust dose; missing it means you trade visceral fat for an insulin problem.
- Stopping cold without a plan. VAT regrows after tesamorelin cessation in trial populations. The discontinuation plan is part of the protocol: diet, training, and a maintenance peptide pattern (often a smaller pulsatile dose) determine whether the gains hold.
- Sourcing low-quality tesamorelin. The ratio of underdosed grey- market vials in this compound class is meaningful. IGF-1 bloodwork at week 6 is the practical assay - if IGF-1 hasn’t climbed at all, the compound is the problem, not the user.
Monitoring on this protocol
- Imaging. DEXA at baseline, week 12, and week 26 is the gold- standard monitoring tool. MRI or CT for VAT is more accurate but more expensive; waist-to-hip ratio is a reasonable poor-man’s proxy when imaging isn’t available.
- Waist circumference. Weekly. The earliest non-imaging signal that the protocol is working - visceral fat reduction shifts waist before total weight on most timelines.
- IGF-1. Baseline and at 6 weeks confirms the GH-axis lever is actually working. A stalled IGF-1 on tesamorelin usually points to underdosed compound or a sourcing issue.
- HbA1c, fasting glucose. Quarterly. The insulin-sensitivity drift risk is the main downside to monitor.
- Lipids, CBC. Baseline and quarterly. Standard for any GH-axis protocol; see Bloodwork for Peptide Users.
- Photographs. Day zero plus monthly. VAT changes show up in profile silhouettes before they show up on the scale.