Insulin shows up everywhere in peptide protocols and almost never on its own page. The fasting-window rule for GH-axis stacks is a fragment of one story; HGH-driven glucose drift is a fragment of another; the GLP-1 muscle-preservation conversation is a fragment of a third. This article puts them on one page, because the underlying question - how endogenous and exogenous insulin interact with every major peptide class - is the same question with different exposures.
Why insulin matters in any peptide protocol
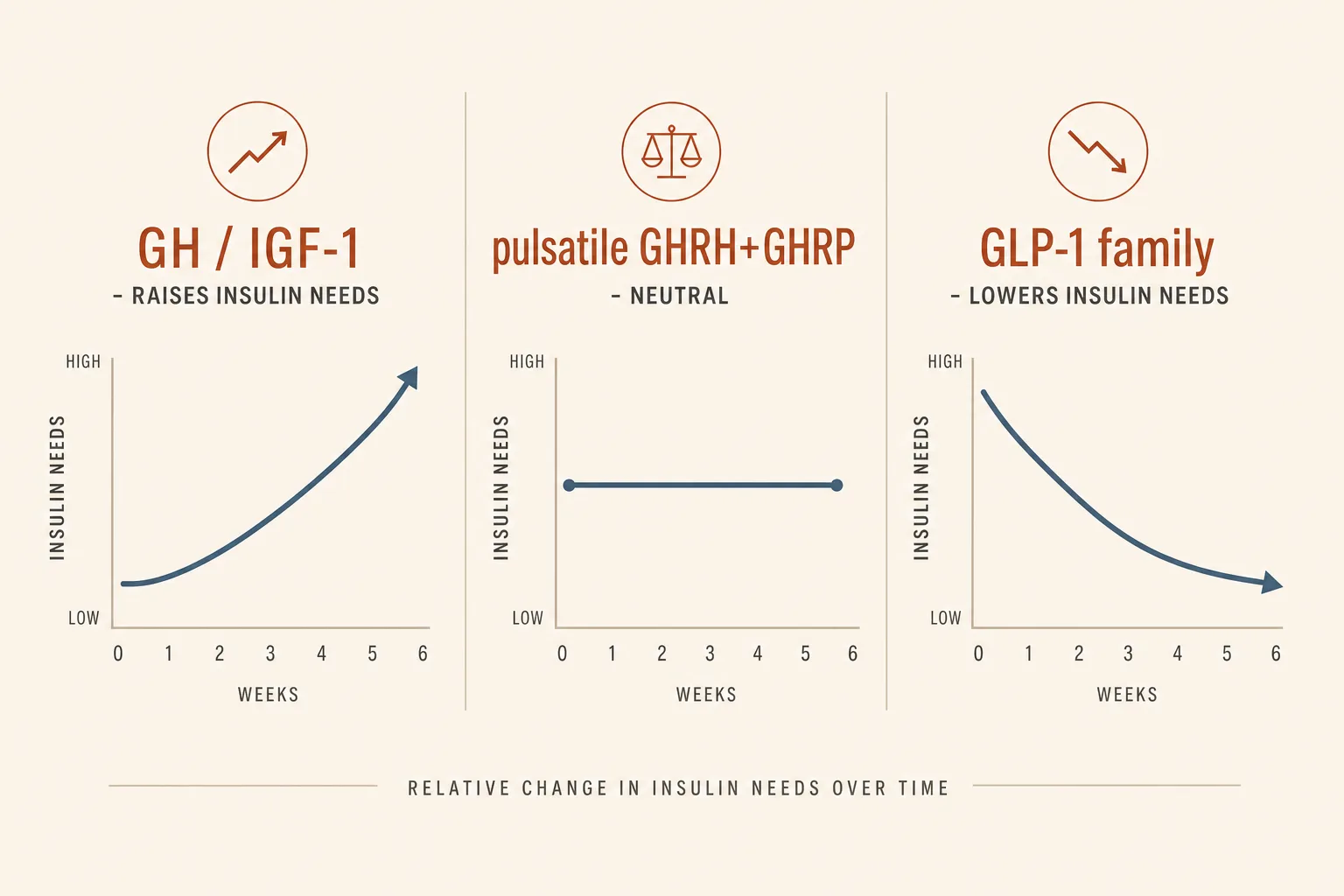
Insulin is the dominant anabolic and storage signal. It opposes lipolysis, blunts growth-hormone release at the pituitary, drives amino acids into muscle, and sets the metabolic ceiling on how much any single peptide can do for body composition. Three relationships show up across the catalog:
- Insulin blunts GH release. Hyperinsulinemia raises somatostatin tone, which shuts the GH pulse the GHRH analog is trying to trigger. Eating and dosing a GHRH at the same time cancels most of the protocol.
- GH and IGF-1 raise insulin resistance. Exogenous HGH, IGF-1 LR3, and continuous-elevation GHRH stacks (CJC-1295 DAC) push fasting glucose and HbA1c upward over a cycle. Native dose pulses recover; sustained elevation drifts.
- GLP-1 receptor agonists lower insulin needs. Semaglutide, tirzepatide, and retatrutide enhance glucose-dependent insulin secretion and improve peripheral sensitivity. For users on exogenous insulin (T1D, T2D), incretin therapy reduces total insulin requirement, sometimes substantially.
These three rules are non-controversial physiology. The complications start when a user is running compounds from more than one of these buckets simultaneously - which is the routine state for the body-hacking-space audience this site is written for.
The fasting-window rule, decoded
Every GH-axis protocol opens with the same instruction: dose on an empty stomach, no food for 30 minutes after. The reason isn't ritual. Insulin is the proximate brake on the GH pulse:
- Carbohydrate hits the gut, glucose rises, beta cells release insulin.
- Insulin signals to the hypothalamus, which raises somatostatin output.
- Somatostatin reaches the pituitary and suppresses the GH pulse that the GHRH analog (Mod GRF, Tesamorelin, sermorelin) is trying to trigger.
- The Ipamorelin layered on top, which works by amplifying that same pulse and inhibiting somatostatin, has less to amplify.
Practical consequence: a user who eats 30 minutes before the pre-bed Mod GRF + Ipamorelin shot has burned the protocol. Subjective effect drops; IGF-1 movement at 6 weeks underperforms expectations; the user blames the peptide. The bigger the carbohydrate load and the closer to the dose, the larger the suppression. Protein-only meals produce a smaller insulin response than mixed meals; a clean fasted state is the only condition that doesn't introduce a variable.
The 30-minute post-dose window matters less than the 2-hour pre-dose window - by the time the GHRH and GHRP have triggered the pulse, the wave has fired and food is no longer load-bearing on the outcome.
Peptides that raise insulin resistance
- Somatropin (rHGH). The clearest signal. Insulin resistance scales with dose and duration. Bodybuilding doses (4+ IU/day) typically push HbA1c by 0.3–0.6 percentage points over a 12-week cycle in users with normal baseline metabolic health, and more in those with insulin resistance already brewing. Often paired with insulin in AAS-context stacks specifically because the HGH-induced resistance has to be compensated.
- IGF-1 LR3. Suppresses fasting glucose acutely (an insulin-mimetic effect) but produces compensatory insulin resistance over weeks at hypertrophy doses. The hypoglycemia risk is real on the first few doses; the metabolic-drift risk is real over a cycle.
- CJC-1295 (DAC). Continuous GH elevation produces the same insulin-resistance pattern as exogenous HGH at lower magnitude. The non-pulsatile signature is what makes it more glucose-disrupting than pulsatile GHRH stacks.
- Tesamorelin. Mild fasting-glucose drift in some users, generally less than CJC-DAC because the pulse architecture is preserved. The Phase 3 trials showed a small HbA1c drift that was offset by the visceral-fat reduction.
- Mod GRF + Ipamorelin (pulsatile stack). Minimal glucose impact at standard doses. The pulse-and-clear architecture is the entire point. Users who break this with sustained doses or constant DAC overlap re-introduce the drift.
Peptides that lower insulin needs
- Semaglutide / tirzepatide / retatrutide. Clinically meaningful reduction in fasting glucose and HbA1c independent of weight loss. For T1D users on basal-bolus regimens, titrating onto incretin therapy without dose-adjusting basal insulin is a fast path to hypoglycemia. The dose adjustment is typically 10–20% basal reduction at GLP-1 initiation, with further titration as the GLP-1 dose escalates. Tirzepatide's GIP component adds an additional sensitivity component beyond the GLP-1 path.
- Liraglutide. Same mechanism, shorter half-life, smaller magnitude. Daily dosing means the dose-adjustment math has more time-resolution than once-weekly compounds.
The body-hacking stack: AAS + insulin + peptides
In the AAS-adjacent end of the audience this site is written for, exogenous insulin is sometimes part of the stack - typically short-acting (Humalog, Novolog) dosed peri-workout, used to drive carbohydrate and amino acids into muscle during a hypertrophy phase. Adding peptides into that stack changes the math:
- Insulin + HGH together. Both are anabolic; both affect glucose; the HGH-induced resistance is partly why insulin is on the stack in the first place. The combination magnifies hypoglycemia risk during the post-injection window if the carbohydrate side of the equation is mistimed. Most operator deaths in this space track to insulin dose-and-timing errors, not HGH errors.
- Insulin + IGF-1 LR3 together. Stacked acute glucose-lowering effect. The first co-dose is the highest risk window. Users who pair them typically separate the IGF-1 LR3 dose from any insulin pin by at least several hours, and never on the same training session.
- Insulin + GLP-1. The GLP-1 reduces insulin requirement; running both at fixed doses without down-titrating basal insulin is the standard mistake. Hypoglycemia in this combination is usually preventable with disciplined titration.
- Insulin + Mod GRF + Ipamorelin. Less risky than the heavier combinations above, but the GH-axis stack should still be dosed in a fasted window separate from any insulin administration. The fasting-window rule for GH-axis becomes a safety rule once exogenous insulin is in play.
This article is not an insulin-protocol guide - that's a separate topic with its own learning curve. But the rule for adding peptides to an insulin-using stack is consistent: every peptide that affects glucose handling shifts the insulin-dose math, and every peptide that requires a fasted window adds a timing constraint to an already-tight schedule.
Practical timing rules
| Compound | Glucose effect | Timing rule | Bloodwork sentinel |
|---|---|---|---|
| Mod GRF + Ipamorelin | Neutral at standard doses | Fasted, ≥2 h post-meal, no food 30 min after | IGF-1 at 6 weeks (efficacy) |
| CJC-1295 (DAC) | Mild-to-moderate drift over weeks | Day-of-week timing low-stakes; cycle length matters | HbA1c at baseline + 12 weeks |
| Tesamorelin | Mild drift | Fasted preferred, less critical than Mod GRF | HbA1c, fasting glucose |
| Somatropin (HGH) | Substantial drift at bodybuilding doses | Morning fasted is the standard slot; insulin-using users co-time with their bolus pattern | HbA1c, fasting glucose, insulin (calc HOMA-IR) |
| IGF-1 LR3 | Acute drop, longer-term resistance | Pre-workout with carbohydrate; never fasted on first dose | Fasting glucose pre-cycle, insulin, HbA1c |
| Semaglutide / tirzepatide / retatrutide | Lowers requirement | Once-weekly, food timing irrelevant; titrate insulin down at each step-up | HbA1c, fasting glucose |
| AOD-9604 / Fragment 176-191 | Neutral; insulin blocks the lipolytic effect | Strictly fasted morning; eat ≥30 min after | None directly; bodyfat trajectory is the signal |
Bloodwork to catch drift early
- Fasting glucose at baseline, 6 weeks, and 12 weeks for any GH-axis protocol. The cheapest, most-informative early signal. A 12-hour fast is the standard prep.
- HbA1c for any cycle longer than 8 weeks. Catches the gradual drift fasting glucose may miss on a single morning. Pre-cycle baseline plus end-of-cycle is the minimum.
- Fasting insulin on long stacks (CJC-DAC + HGH, or hypertrophy-tier IGF-1 LR3 cycles). Combined with fasting glucose, calculate HOMA-IR ([fasting insulin × fasting glucose] / 405 in mg/dL units, or / 22.5 in mmol/L). Above 2.5 means something has shifted.
- OGTT (oral glucose tolerance test) for users on HGH or DAC for >6 months, especially with family history of T2D. The post-load number sometimes drifts before fasting numbers do.
- Continuous glucose monitor (CGM) for 14 days at cycle midpoint is increasingly the preferred operator tool - it catches post-prandial spikes that point-measurements miss, and the cost has dropped to roughly the price of a bloodwork panel.
What stops people
- Eating before the pre-bed GH-axis dose. The single most common protocol error. The "I just had a small snack" user is running a quarter-strength stack and not knowing it.
- Stacking IGF-1 LR3 fasted on the first day. Hypoglycemia is real and the first dose is the highest-risk window. Pre-load carbohydrate, dose with food, gauge response over the first three sessions before adjusting.
- Adding GLP-1 to an existing insulin regimen at fixed insulin dose. The GLP-1 reduces insulin need; not titrating basal down at GLP-1 initiation produces the hypoglycemia that gets blamed on the GLP-1 itself.
- Running CJC-DAC year-round. The continuous elevation drives the metabolic drift. Cycling - 8 weeks on, 4 weeks off, or seasonal - limits the damage. See Cycling Strategies.
- Skipping the HOMA-IR calculation. Fasting glucose alone misses early insulin-resistance drift; the panel isn't expensive but the calculation almost never gets done.
- Combining HGH and exogenous insulin without a CGM in the loop. Two strong glucose-affecting compounds need feedback that point-measurements don't provide. The CGM has become the standard tool here, not a luxury.
Cross-references
- GH Axis Playbook - the per-compound mechanism story; this article is the metabolic overlay.
- Bloodwork for Peptide Users - the broader panel discussion that includes the glucose / insulin sentinels above.
- Semaglutide vs Tirzepatide vs Retatrutide - the per-compound profile when GLP-1 is the lowering side of this equation.
- GLP-1 and Muscle Preservation - the related discipline question for users in a calorie deficit alongside the insulin shift.
- Cancer Risk and Growth Factors - the longer-arc question on sustained IGF-1 elevation, where the insulin pathway also matters.
- Peptides on Top of an AAS or TRT Stack - the broader combined-stack decision tree the AAS+insulin section above lives inside.
What this article doesn't cover
Specific exogenous-insulin protocols - basal/bolus ratios, carb-counting, peri-workout dosing - are out of scope. That's a diabetes-management or AAS-protocol topic and merits its own treatment by people closer to it. Insulin sensitisers (metformin, pioglitazone) and their interaction with peptide protocols are also separate; the relevant points are noted in Cancer Risk and Growth Factors rather than expanded here.