Resting heart rate is the easy sentinel - one number, off any cheap wrist tracker, trends linearly with most catalog protocols. Blood pressure is the harder sentinel and the more useful one. It moves in different directions for different classes, drifts on different timescales, and the gap between a clinic reading and a real home baseline is wide enough that single measurements are mostly noise. The Heart Rate as a Peptide Sentinel piece is the companion; this article is the BP half of the same physiological story.
Why blood pressure moves at all
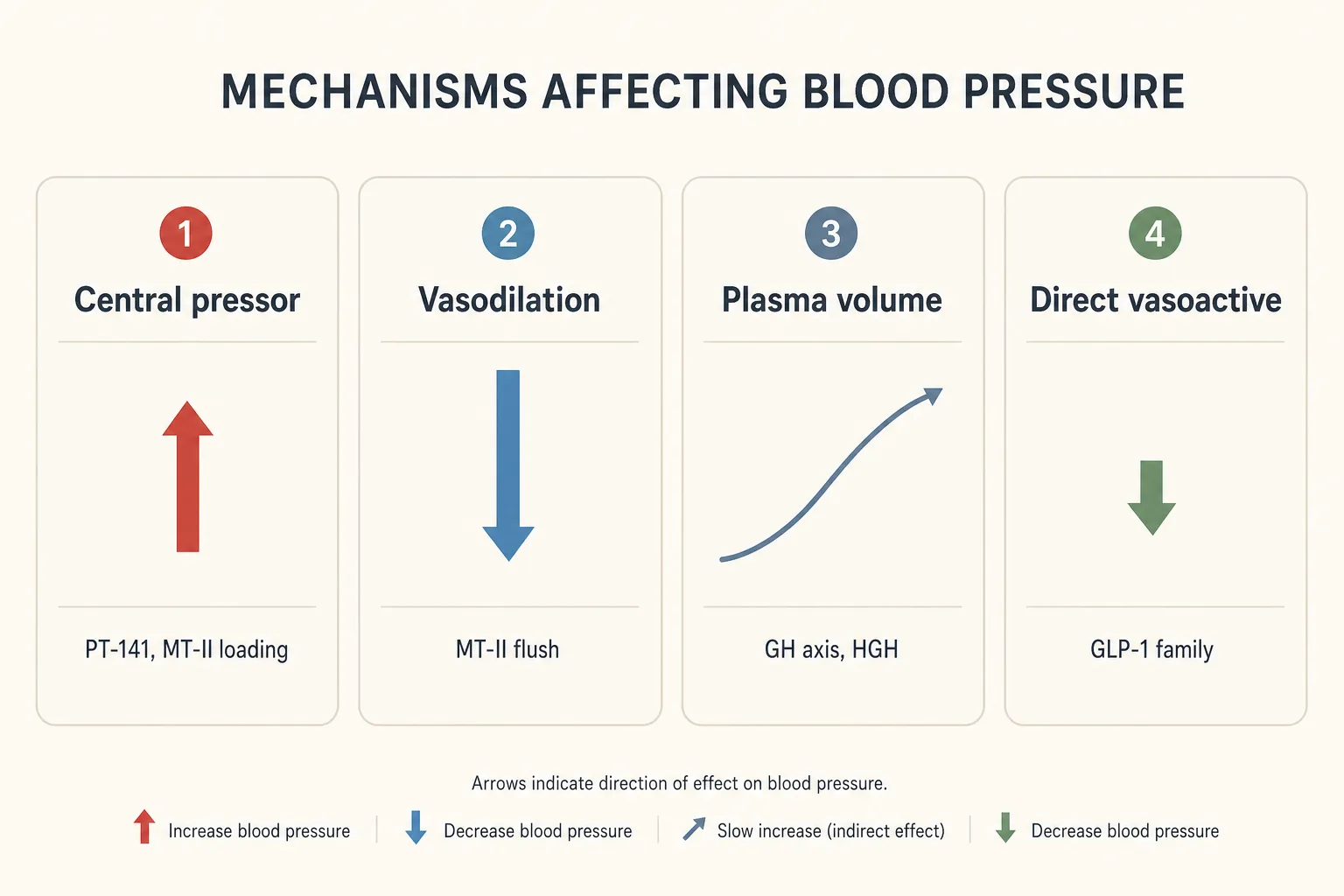
Four mechanisms account for almost everything you'll see across this catalog:
- Acute central pressor effect. Melanocortin activation (PT-141, MT-II loading doses) triggers a transient sympathetic surge that raises systolic BP for 1-6 hours after dosing. The effect is dose-dependent and habituates partially with repeat exposure.
- Vasodilation and flush. Higher MT-II doses and several other peptides produce cutaneous vasodilation - the visible flush is the signal. In susceptible individuals this can drop systolic BP by 10-15 mmHg for 30-60 minutes, particularly in the upright position.
- Plasma volume expansion. GH-axis stacks that drive water retention (CJC-1295 DAC, exogenous HGH at bodybuilding doses) expand plasma volume. The result is a slow climb of 3-8 mmHg systolic over the first 2-4 weeks of a protocol, which reverses on washout.
- Modest direct vasoactive effect. GLP-1 family peptides produce a small, consistent BP drop independent of weight loss - mechanism is debated (NO signaling, natriuresis, modest sympathetic dampening), but the effect is reproducible across trials.
None of these mechanisms produces dramatic numbers in a healthy user. The point of measuring isn't catching emergencies - it's catching drift early in the population that matters: pre-hypertensive users, GH-axis stackers running multi-month cycles, anyone with a family cardiovascular history.
Per-class baseline expectations
| Compound | Typical BP shift on protocol | Mechanism | Reverses? |
|---|---|---|---|
| Semaglutide (titrated to 2.4 mg) | -3 to -5 mmHg systolic | Direct GLP-1 vasoactive + weight-loss compounding | Yes, on discontinuation; weight-loss component lags |
| Tirzepatide (15 mg) | -5 to -8 mmHg systolic | GIP/GLP-1 dual agonism; larger weight-loss component | Yes, on discontinuation |
| Retatrutide (high-dose Phase 2 arms) | Variable: -3 to +5 mmHg | Glucagon-receptor pressor competing with weight-loss offset; net effect is individual | Yes, on washout - but watch the trend |
| PT-141 (Vyleesi, on-demand) | +5 to +10 mmHg systolic, 1-6 h post-dose | Acute MC4R-mediated sympathetic activation | Yes, returns to baseline within 6-12 h |
| MT-II (loading dose) | +5 mmHg systolic on the pressor side, then -5 to -10 mmHg during flush | Central pressor competing with cutaneous vasodilation | Yes, the same dose has less BP signal after the loading phase |
| MT-II (maintenance dose) | Minimal at-rest shift; pressor and dilator effects both attenuated | Habituation | N/A |
| CJC-1295 DAC (continuous-elevation GH) | +3 to +6 mmHg systolic over 2-4 weeks | Plasma-volume expansion, water retention | Yes, on washout (typically 2-3 weeks to baseline) |
| Mod GRF 1-29 + Ipamorelin (pulsatile) | Minimal direct BP effect | Pulsatile profile spares the plasma-volume mechanism | N/A |
| Tesamorelin | Minimal direct BP effect; visceral-fat loss can lower BP indirectly over months | Pulsatile GHRH; no continuous-elevation pathway | Yes, on discontinuation - visceral fat returns |
| Exogenous HGH (bodybuilding doses, 4+ IU/day) | +5 to +10 mmHg systolic over 4-8 weeks | Plasma-volume expansion + IGF-1-mediated sodium retention | Slowly, on washout |
| BPC-157, TB-500, GHK-Cu, KPV | No reliable direct BP effect | None of these classes engages BP-relevant pathways | N/A |
| IGF-1 LR3 / DES / PEG-MGF | Minimal at-rest shift; can lower BP transiently via glucose drop | Insulin-like glucose handling, not a direct vasoactive effect | Acute, not protocol-level |
| Thymosin Alpha-1, Thymosin Beta-4 (systemic) | No reliable BP effect | Immune-axis, not cardiovascular | N/A |
Why home cuff beats clinic reading
A single clinic BP reading is a noisy sample of a noisy signal. Three problems compound:
- White-coat effect. 15-25% of users register systolic readings 10-20 mmHg higher in clinic than at home, with the same true baseline. For peptide users at the edge of normal range, this is the difference between "fine" and "hypertensive" on paper.
- Time-of-day variation. BP follows a circadian rhythm with a 5-15 mmHg amplitude. A morning reading and an afternoon reading can disagree by more than the protocol's expected drift.
- Cuff fit and posture. Wrong-size cuffs (most "one-size" cuffs run too small for muscular forearms or large upper arms) over-read by 5-10 mmHg. Crossed legs, unsupported back, or talking during the measurement add another 5-8 mmHg.
The protocol that beats clinic readings: a validated upper-arm oscillometric cuff (the Omron 7-series and equivalents are the cheap-and-fine standard), measured twice in the morning and twice in the evening, seated quietly for 5 minutes, feet flat, arm at heart level, supported. Average across a week. That number is closer to truth than any clinic reading.

Postural readings: the cheap test most users skip
Postural (orthostatic) blood pressure - taken seated and again standing - catches a different problem: vasodilation-driven dizziness and the early signal of GLP-1 dehydration. The protocol:
- Sit quietly for 5 minutes; take a baseline reading.
- Stand up; wait 1 minute; take a second reading.
- Wait another 2 minutes standing; take a third reading.
A drop of more than 20 mmHg systolic or 10 mmHg diastolic on standing is the classical orthostatic-hypotension threshold. For peptide users this is the test that catches:
- GLP-1 users with insufficient fluid intake (the appetite suppression cuts thirst signaling too).
- MT-II loaders during the active flush window.
- Users on combined GLP-1 + antihypertensive medication where the GLP-1 BP drop stacks unintentionally on top of an existing regimen.
The 14-day baseline before any new protocol
The first useful number isn't the protocol-day BP - it's the pre-protocol baseline you collected over the two weeks before starting. Without it, every drift is a guessing game about whether it was already there. The discipline:
- 14 days, twice-daily home cuff readings (morning + evening), same conditions each time.
- Average. That's the baseline systolic and diastolic to compare against.
- Note the variability range - if your baseline range is 115-130 systolic, a single 134 reading on protocol means nothing. A run of seven 132+ readings does.
The same logic applies to the heart-rate sentinel - see Heart Rate as a Peptide Sentinel for the parallel discipline. Most users who do one will do the other; the cuff and the wearable answer different questions but they share the daily-measurement habit.
Stop signals - by class
| Class | Stop / pause threshold | What to do first |
|---|---|---|
| GLP-1 family | Postural drop >20 mmHg, or symptomatic lightheadedness on standing | Increase fluid + salt intake; if it persists for a week, hold the next dose escalation |
| PT-141 | Sustained reading >160/100 in the 2-6 h post-dose window, or any reading triggering symptoms (chest pressure, severe headache) | Discontinue. The on-demand model means a single bad response is enough data; this isn't a "titrate down" drug. |
| MT-II | Sustained pressor signal during loading - reading consistently above pre-protocol baseline +10/+5 mmHg, or symptomatic flushing with significant BP drop on standing | Slow the loading schedule; reduce per-dose to 250 mcg and retest after 1 week. |
| GH-axis (CJC DAC, HGH) | Sustained climb of >10/6 mmHg over 4-week baseline, or new-onset edema combined with any BP drift | Pause the protocol. If the drift was edema-driven, baseline returns within 2-3 weeks of washout. Reassess before resuming. |
| Retatrutide | Sustained >10 mmHg systolic above 14-day baseline, especially if accompanied by HR climb | Pause titration. If both HR and BP are climbing, this is a reason to drop dose, not just hold. |
| Any class, any reading >180/120 | Hard stop regardless of cause | This is hypertensive-urgency territory. Get it checked clinically; the peptide question can wait. |
Concurrent antihypertensives: the unspoken interaction
A meaningful fraction of the audience here is on existing BP medication - ACE inhibitors, ARBs, calcium-channel blockers, beta-blockers, thiazide diuretics. The peptide protocol doesn't exist in isolation; it interacts with that floor:
- GLP-1 + ACE/ARB: additive BP drop, especially in the first month of titration. Monitor postural readings; the fix is usually a small dose reduction of the antihypertensive, not stopping the GLP-1.
- GLP-1 + thiazide: the dehydration component of aggressive GLP-1 titration stacks with the thiazide's diuretic effect. Sodium and fluid status matter; this is the user who actually needs to drink more, not less.
- PT-141 + beta-blocker: the beta-blocker blunts the acute pressor response, which is helpful, but the rebound off the beta-blocker cycle (if the user is between doses) can leave the PT-141 effect unopposed. Time the dose with the beta-blocker.
- GH-axis + any antihypertensive: the plasma-volume mechanism doesn't respond evenly to all antihypertensive classes. Diuretics and ARBs help; beta-blockers are roughly neutral; calcium-channel blockers don't change the fluid component much.
What stops people
- Skipping the pre-protocol baseline. The single most common failure. Without 14 days of pre-protocol data, every on-protocol number is interpreted in a vacuum.
- Trusting one bad reading. BP is noisy. A single 145/95 means almost nothing; seven of them in a row means something. Average a week before deciding.
- Wrong cuff size. The factory cuff that comes with cheaper monitors fits maybe 60% of adult upper arms. Measure your arm circumference once and buy the correct cuff size; it's a 10-minute fix that eliminates a 10 mmHg systematic error.
- Measuring in the wrong window. An evening reading after caffeine, alcohol, or a hard training session is not your baseline. Standardize the window.
- Treating the clinic reading as authoritative. For peptide-protocol decision-making, the home cuff average is the data. Bring the home log to the clinic, not the other way around.
Sources
- SURMOUNT-1 trial (tirzepatide weight loss, BP secondary endpoint) - Jastreboff et al., NEJM 2022 - https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
- STEP-1 trial (semaglutide, BP secondary endpoint) - Wilding et al., NEJM 2021 - https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
- Retatrutide Phase 2 (Jastreboff et al., NEJM 2023) - https://www.nejm.org/doi/full/10.1056/NEJMoa2301972
- Vyleesi (bremelanotide) FDA label, BP precaution section - https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
- AHA Home BP Monitoring guidance - https://www.heart.org/en/health-topics/high-blood-pressure/understanding-blood-pressure-readings/monitoring-your-blood-pressure-at-home
Cross-references
- Heart Rate as a Peptide Sentinel - the companion article on the cardiac half of the same physiology.
- Bloodwork for Peptide Users - the broader monitoring framework BP and HR sit inside.
- Cancer Risk and Growth Factors - the parallel cumulative-exposure frame for a different system.
- PT-141, Melanotan II, CJC-1295 DAC, Retatrutide, Tirzepatide, Semaglutide - the catalog pages for the compounds with the largest BP signatures.
- Peptides and Aging - the 50+ population where the cardiovascular sentinels matter most and where pre-existing antihypertensive regimens are common.