Sleep is the application most prone to user-discipline confounds. Anyone with poor sleep hygiene, late caffeine, irregular schedule, alcohol, blue-light exposure at midnight, or undiagnosed apnoea will get more from fixing those than from any peptide on this page. With that frame, three compounds have a real lever: pre-bed Ipamorelin is the cleanest practical one, DSIP is the responder-variance experiment, and Epitalon sits in the speculative cycle-based bucket.
The shortlist by approach
Pre-bed Ipamorelin (or full GH-axis stack)
- What it does. A pre-bed Ipamorelin pulse aligns with the natural nocturnal GH peak and deepens it. Users consistently report deeper sleep within the first week, sometimes with vivid dreams in the first 3–5 nights as REM architecture adjusts. The body-comp / recovery returns are the side benefit; the sleep effect is the primary one for this application.
- Mechanism. GH itself doesn’t directly induce sleep, but a deeper nocturnal GH pulse correlates with more slow-wave sleep in human studies. Whether it’s causal or parallel is not fully resolved; the practical result is consistent.
- Protocol. Ipamorelin 100–200 mcg SC, 15–30 min before bed, fasted (2+ hours after last meal). Add Mod GRF 1-29 100 mcg if recovery / body-comp is also a goal. Full runbook in the Pre-Bed GH-Secretagogue Protocol guide.
- Where it fits. Default first-line for sleep quality. Lowest side-effect surface in this entire application.
DSIP - delta sleep-inducing peptide
- What it is. A 9-amino-acid peptide originally isolated from rabbit cerebral venous blood (Schoenenberger 1977), associated with delta-wave (slow-wave) sleep induction. Half-life is short - 15 minutes plasma, but the proposed mechanism is via sleep-onset signalling rather than sustained sedation.
- Evidence framing. Tier: Limited data. The early animal and small clinical literature is mixed; modern replication is thin. Community use is real and there’s a genuine subset of consistent responders. There’s also a genuine subset of complete non-responders.
- Protocol. 100–250 mcg SC, 1–3 hours before bed, not at bedtime. Timing is the load-bearing variable: dosed too late (right at bedtime), DSIP can paradoxically cause alertness in some users. Dosed early evening, it produces a wind-down effect.
- Where it fits. A 2-week experiment for users who have fixed the basics, run pre-bed Ipamorelin, and still want a sleep-onset lever. Stop if no clear effect after the trial - the responder/non-responder split is real and a 4-week trial won’t change a 2-week null.
Epitalon - cycle-based circadian framing
- What it is. A 4-amino-acid synthetic version of Epithalamin, an extract from bovine pineal gland. Researched primarily by Khavinson and colleagues in St. Petersburg over the 1990s–2010s. Claimed mechanism is melatonin / pineal upregulation and telomerase induction.
- Evidence framing. Tier: Limited data. The Khavinson long-term mortality studies are the largest body of evidence and are largely Russian-language, with replication scarcity in Western literature. Telomerase claims are particularly uncertain.
- Protocol. Two patterns in community use. The Khavinson original: 10 mg/day SC or IM for 10 days, repeated every 6 months. The modern low-dose alternative: 100–500 mcg/day for longer durations. The latter deviates from the primary evidence base.
- Where it fits. Speculative tier. For users who already have Ipamorelin and DSIP dialled and want a cycle-based longevity-adjacent intervention. Don’t expect acute sleep improvement; the framing is circadian / longer-horizon.
Selank / Semax - the wrong tools for sleep
Worth flagging because they’re sometimes recommended in this context: Selank and Semax are nootropic / anxiolytic peptides with mild dopaminergic and BDNF effects. They can reduce racing thoughts that prevent sleep onset in users with anxiety-driven insomnia - that’s real. They are not sleep peptides per se; if the limiter is anxiety, they help; if the limiter is anything else, they don’t.
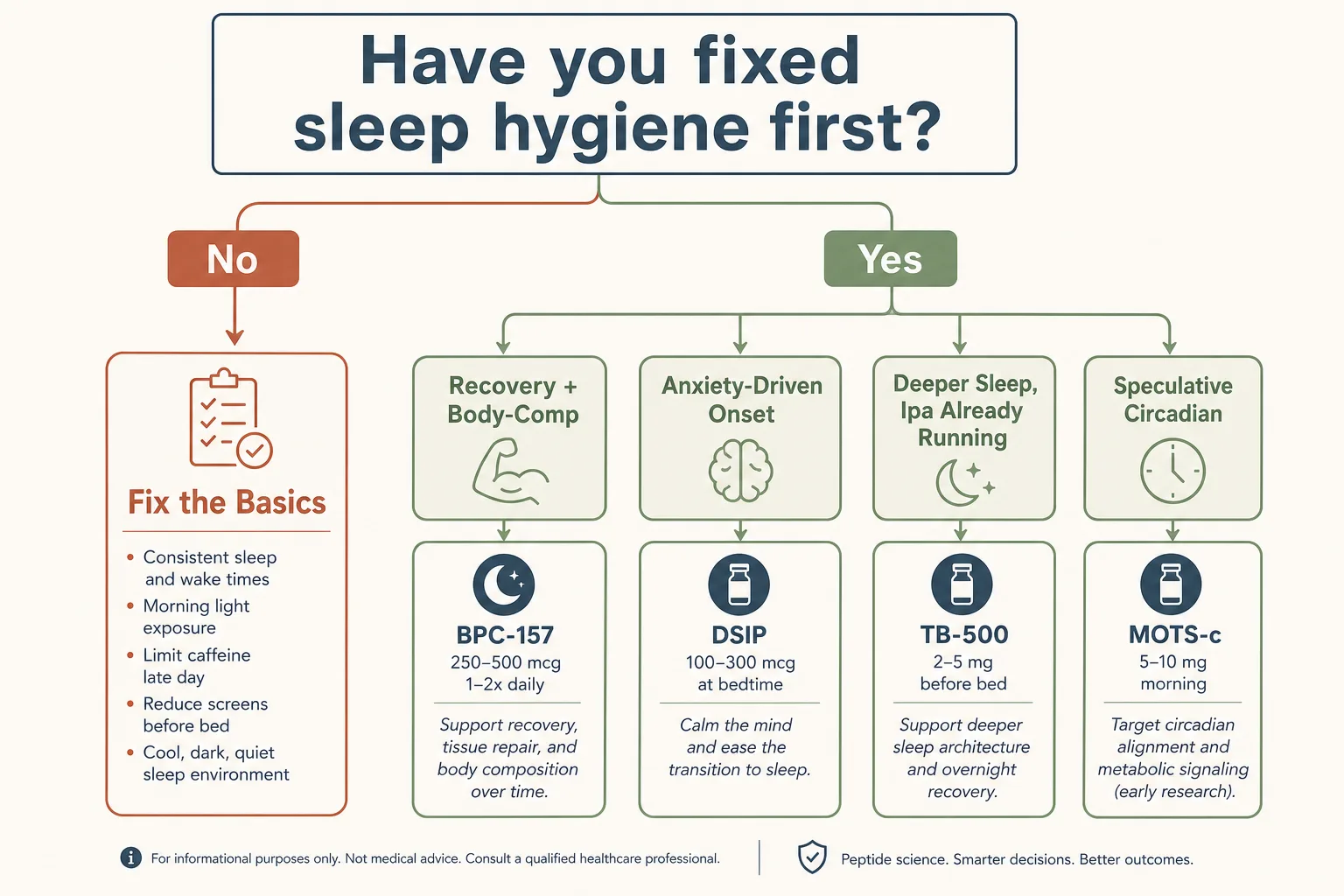
Decision guide
- Have you fixed sleep hygiene first?
→ If not, peptides are the wrong layer. Caffeine cut-off by 2 PM, screens out an hour before bed, regular schedule, room temperature 18–20°C, blackout curtains. None of the compounds below will rescue a structurally bad sleep environment. - Sleep apnoea screening done?
→ Particularly important if running GH-axis protocols - untreated apnoea + GH stack can worsen the apnoea. Snoring, daytime sleepiness, witnessed apnoeas: get screened before adding any compound to the picture. - Goal: deeper sleep + recovery + modest body-comp?
→ Ipamorelin pre-bed (or full Mod GRF + Ipa stack). Start here. - Goal: better sleep onset, anxiety-driven racing
thoughts?
→ Selank evening dose (250 mcg intranasal) is a reasonable experiment. Not a sedative; addresses the anxiety contributor. - Goal: deeper sleep, Ipamorelin already running?
→ 2-week DSIP trial 1–3 hours pre-bed. Stop if no effect. - Goal: speculative circadian / longevity framing?
→ Epitalon Khavinson protocol once or twice a year. Don’t expect acute sleep improvement.
Representative stacks
Stack 1 - Sleep + recovery default
- Ipamorelin 100–200 mcg SC, 15–30 min pre-bed, fasted
- Optional: Mod GRF 1-29 100 mcg paired in the same syringe (use the Pre-Bed GH-Secretagogue Protocol)
- Sleep journal week 1–4 to track subjective change against objective sleep tracker if available
Stack 2 - DSIP responder experiment
- Stack 1 base running for 4+ weeks first to isolate the DSIP variable
- DSIP 200 mcg SC, 1–3 hours pre-bed (not at bedtime), 14 days
- Sleep tracker / journal during the 14 days, comparing to baseline at end of week 2
- If no clear effect, stop. If responder, taper to alternate-day or use as needed.
Stack 3 - Anxiety-driven sleep onset
- Selank 250 mcg intranasal, evening (1–2 h before bed)
- Optional: Stack 1 base for the GH-axis benefit on top of the onset support
- Reassess at 4 weeks - Selank shouldn’t be needed chronically if the anxiety driver resolves
What stops people
- Skipping sleep hygiene and stacking compounds. The single most common pattern in user reports of "peptides didn’t help me sleep". Hygiene first; peptides are the marginal lever, not the foundation.
- Mistiming DSIP. Dosing right at bedtime instead of 1–3 hours before is the most common DSIP user error. Late DSIP can produce alertness in a chunk of users - the opposite of the goal.
- Treating Epitalon as a sleep peptide. The framing is circadian / longevity. Acute sleep improvement is not the typical effect; expecting it produces disappointment.
- Stacking sedatives + DSIP + alcohol. The interactions aren’t well-characterised but the pattern of additive sedation is plausible. Pick one CNS depressant per night.
- Ignoring the GH + apnoea interaction. If snoring is an existing pattern, GH-axis protocols can worsen it. Sleep study before stacking the protocol if there’s any suspicion.
Monitoring
- Sleep tracker (wearable or app). Total sleep time, deep-sleep fraction, sleep latency. Imperfect but the cheapest objective signal.
- Sleep journal. Subjective rest quality 1–10, morning fatigue, daytime energy. The wearable misses what the journal catches.
- Resting heart rate. Trends downward with better recovery; trends upward with overtraining or undersleeping.
- IGF-1 + HbA1c quarterly if running GH-axis protocols. Standard for any sustained GH-axis work; see Bloodwork Panel Cheat Sheet.
Cross-references
- GH Axis Playbook - the deeper article on Ipamorelin / Mod GRF and where the pre-bed dose fits.
- Pre-Bed GH-Secretagogue Protocol - the runbook for Stack 1.
- Injury Recovery application - the broader recovery framework.
- Cycling Strategies - the on/off rationale for the GH-axis stack.