What ratio-based dosing means
A blended vial is a fixed-proportion mixture: each component has a set fraction of the total content, locked at the moment of formulation. Once reconstituted, the only handle you have is the draw volume - and that draw pulls every component out together, in the original ratio. Pick the "driver" dose for one peptide; the rest follow automatically.
This is convenient when the partner peptides have similar dosing schedules, similar stability, and the ratio itself is the protocol you want. It's a trap when the partners need different cadences, when their stability profiles don't match, or when a tolerability problem with one component forces you to drop the entire blend.

Driver peptide logic
Pick one component as the "driver" - usually the one with the more precise dose target - and let the rest follow.
If a blend contains:
- Peptide A total amount = Atotal
- Peptide B total amount = Btotal
- Chosen dose of A = Adose
Then the B dose implied by the ratio is:
Bdose = (Adose ÷ Atotal) × Btotal
Practical consequence: you cannot change one component independently. To raise A while holding B constant, the only option is to start a fresh vial at a new ratio.
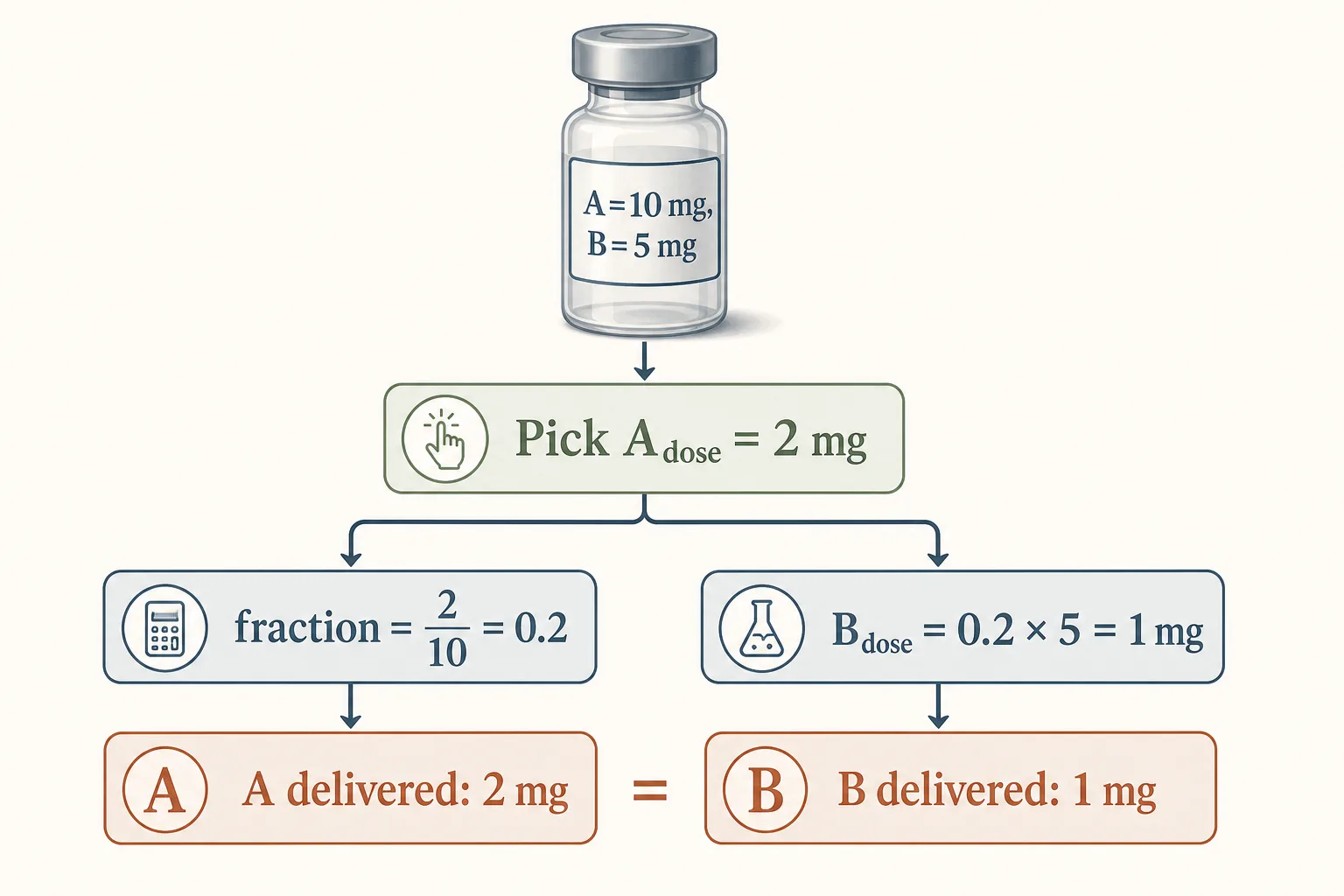
Worked example 1 - simple 2:1 blend
Blend contains A = 10 mg and B = 5 mg total (2:1 ratio). If chosen Adose is 2 mg:
- Fraction of vial used = 2 ÷ 10 = 0.2
- Bdose = 0.2 × 5 = 1 mg
- Reconstituted in 2 mL → A concentration = 5 mg/mL, B = 2.5 mg/mL
- Volume to draw = 0.4 mL (= 2 mg ÷ 5 mg/mL = 1 mg ÷ 2.5 mg/mL - same answer on either path)
Worked example 2 - Mod GRF + Ipamorelin pre-bed blend
Standard pre-bed combo: 5 mg Mod GRF 1-29 + 5 mg Ipamorelin in a single vial reconstituted to 2 mL. Each component is at 2.5 mg/mL = 25 mcg/U. Want 100 mcg of each:
- Driver: Mod GRF 100 mcg → 4 units
- Ipamorelin co-delivered: 100 mcg (because the ratio is 1:1)
- Total draw: 4 units
This blend is convenient because the two compounds share the pre-bed cadence, both target the same fasting-state context, and stability matches over the 28-day window. Standard practice for this stack.
Worked example 3 - when the math breaks down
Suppose someone makes a 5 mg BPC-157 + 5 mg TB-500 blend (1:1, both gut + tendon healing), reconstituted to 2 mL. Want a 250 mcg BPC-157 dose:
- BPC concentration = 2.5 mg/mL = 25 mcg/U
- 250 mcg → 10 units
- TB-500 co-delivered = 250 mcg per dose
- But TB-500 standard dose is 2.5 mg twice weekly, not 250 mcg daily. The blend forces a TB-500 cadence that doesn't match its half-life or pharmacology.
This is what "the blend isn't always the right answer" looks like in practice. The convenience of one injection comes at the cost of running the partner compound on the wrong schedule.
When blending makes sense
- Same dosing schedule. Both compounds run daily, both at the same time of day, both in the same fasted/fed context.
- Similar stability. Both compounds tolerate the same refrigerated 28-day window without one degrading much faster than the other.
- Synergistic mechanism. The combination is the protocol - Mod GRF + Ipamorelin hitting two different receptors on the same pituitary cell at the same pulse window is the canonical example.
- Mature community track record. Pre-formulated blends sold by reputable vendors with consistent ratios across batches.
When blending is a mistake
- Different cadences. Daily compound + weekly compound. Forcing both onto one schedule wastes the weekly compound or sub-doses the daily one.
- Stability mismatch. IGF-1 LR3 (fragile, 14–21 day reconstituted shelf life) blended with BPC-157 (robust, 30–60 days) means the LR3 degradation curve dictates the discard date - you waste BPC. See Cold-Chain Reality for the per-class stability table.
- Different solubility / pH preferences. Some peptides prefer slightly acidic carriers; others neutral. Forcing them into one BAC-water vial accelerates aggregation in the less-tolerant partner.
- Unbalanced dose magnitudes. A 1:50 ratio (e.g. 100 mcg of one compound paired with 5 mg of another) means dose granularity for the small-amount component is poor - small variations in draw volume produce large percentage errors on the smaller component.
- Different evidence tiers. Putting a Clinical-tier compound (Tesamorelin, FDA-approved) in a blend with a speculative-tier compound (MOTS-c, Preclinical) means the speculative tier rides on the clinical compound's protocol cadence. Mixing evidence levels makes response attribution impossible.
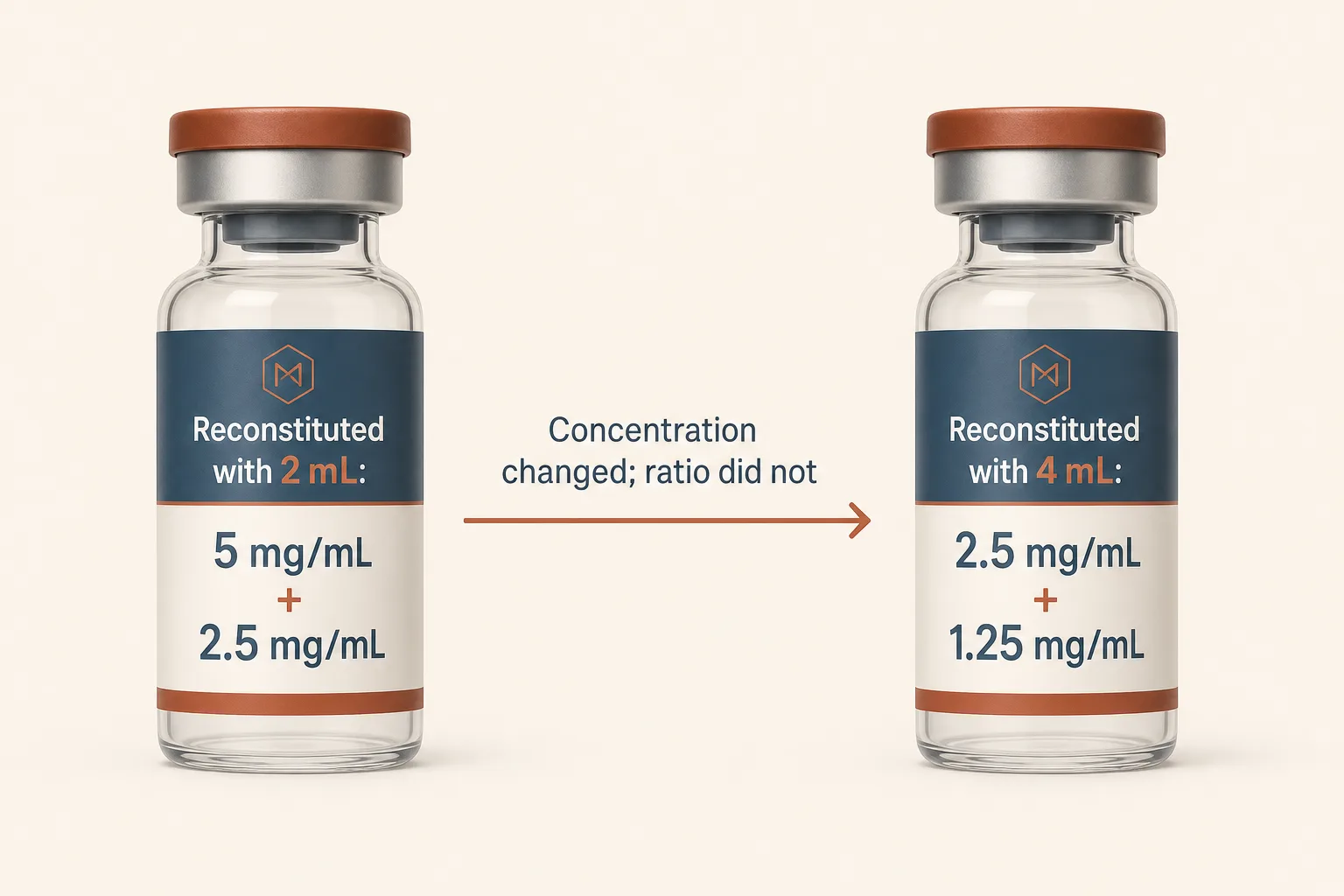
The reconstitution-volume invariant
Changing the BAC water volume changes the per-mL concentration of every component, but doesn't change the ratio. A 5 mg + 5 mg blend at 2 mL gives 2.5 mg/mL of each; reconstituted at 4 mL it gives 1.25 mg/mL of each. The ratio stays 1:1. Use this to land your typical dose on whole insulin-syringe units - same trick as single-component vials, see Reconstitution Cheat Sheet.
Practical harm-minimising checks
- Document exact vial composition. Both component amounts and the date of formulation, on the side of the vial. The blend ratio is invisible from the outside; written records are the only safeguard.
- Run the dose math for each component, not just the driver. The partner dose is not optional information - it's what the user actually receives.
- Avoid ambiguous shorthand. "Wolverine blend" or "GH stack" without the ratio is useless. Always pin the components and amounts.
- Treat combined uncertainty as higher than single-agent. Side-effect attribution gets harder; if something goes wrong, you can't easily separate which compound caused it without stopping the blend and switching to single-component vials.
Common pitfalls
- Forgetting the partner dose. Tracking only the driver in your protocol log loses half the data. Both component doses go in the journal.
- Assuming the ratio shifts with reconstitution volume. It doesn't. Concentration changes, ratio stays.
- Using a "convenient" blend ratio that doesn't match either component's dose-response curve. A 1:1 blend forced because that's what the vendor sells, used at the wrong dose for both compounds.
- Re-reconstituting partway through. Topping up the vial with new BAC water mid-cycle to extend it doesn't extend it - it dilutes both components and confuses every subsequent dose calculation. Reconstitute fresh per cycle.
- Mixing two single-component vials yourself thinking it makes a blend. Mechanically yes, but the resulting "blend" inherits the worse of the two stability profiles, and any contamination in either source vial enters the new shared vial. Pre-formulated blends or single-component vials drawn separately into one syringe are both cleaner approaches.
Sources
- FDA: Drug combinations and fixed-dose products (regulatory framing) - https://www.fda.gov/drugs/development-approval-process-drugs
- ISMP medication safety principles (dose clarity and error prevention) - https://www.ismp.org/recommendations
- CDC Injection Safety basics - https://www.cdc.gov/injection-safety/hcp/clinical-guidance/index.html